E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(2); 2023 > Article
-
Resident fellow section: Teaching images
A 40-year-old man with neuropathic pain in the entire left foot -
Jae Hwa Bae1,*
 , Mathieu Boudier-Revéret2, Min Cheol Chang1
, Mathieu Boudier-Revéret2, Min Cheol Chang1 -
Journal of Yeungnam Medical Science 2023;40(2):223-224.
DOI: https://doi.org/10.12701/jyms.2022.00486
Published online: August 30, 2022
1Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, Daegu, Korea
2Department of Physical Medicine and Rehabilitation, Centre Hospitalier de l’Université de Montréal, Montreal, QC, Canada
- Corresponding author: Min Cheol Chang, MD Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-4682 • Fax: +0504-231-8694 • E-mail: wheel633@gmail.com
- *The first author, Jae Hwa Bae, is currently in training.
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,498 Views
- 59 Download
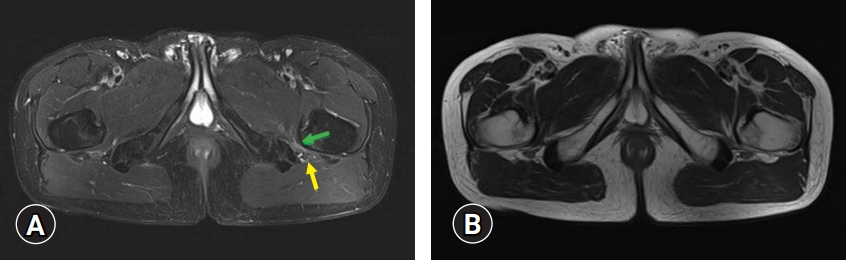
- • Ischiofemoral impingement can cause buttock pain with or without sciatica due to irritation of the adjacent sciatic nerve, which is caused by impingement of the quadratus femoris muscle between the lesser trochanter and lateral border of the ischium.
- • Edema and a narrowed ischiofemoral space identified by pelvic MRI indicate ischiofemoral impingement.
- • For ischiofemoral impingement, conservative treatment with activity modification and ischiofemoral space injection can be attempted. In cases that are refractory to conservative treatment, surgical treatment should be considered.
Learning points
-
Ethical statements
This study was approved by the Institutional Review Board (IRB) of Yeungnam University Hospital (IRB No: 2022-07-029). Written informed consent was obtained for the publication of this report.
-
Conflicts of interest
Mathieu Boudier-Revéret has been editorial board member of Journal of Yeungnam Medical Science (JYMS) since 2021. Min Cheol Chang has been Associate editor of JYMS since 2021. They were not involved in the review process of this manuscript. Otherwise, there is no conflict of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: MBR, MCC; Data curation, Formal analysis, Methodology, Visualization, Investigation, Resources, Supervision, Validation: MCC; Writing-original draft: all authors; Writing-review & editing: all authors.
Notes

- 1. Lee S, Kim I, Lee SM, Lee J. Ischiofemoral impingement syndrome. Ann Rehabil Med 2013;37:143–6.ArticlePubMedPMC
- 2. Ulusoy OL, Tutar S, Ozturk E, Mutlu A, Mutlu H. Ischiofemoral impingement syndrome: another cause of extraspinal sciatica. Spine J 2016;16:e527.ArticlePubMed
- 3. Wilson MD, Keene JS. Treatment of ischiofemoral impingement: results of diagnostic injections and arthroscopic resection of the lesser trochanter. J Hip Preserv Surg 2016;3:146–53.ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite