Playing snakes and ladders with the common fibular nerve on ultrasound after knee dislocation
Article information

We present the case of a 21-year-old previously healthy varsity rugby athlete with left common fibular nerve (CFN) injury following knee dislocation. She presented to a local hospital with a traumatic knee injury following blunt anterior impact causing posterior dislocation. Immediately, she noted anesthesia of the lateral leg and dorsal foot, and dorsiflexion paralysis. Computed tomography revealed a tibial plateau fracture with 2 mm impaction. Magnetic resonance identified torn anterior and posterior cruciate ligaments, a torn lateral collateral ligament, and a grade one medial collateral ligamentous sprain. The fibular nerve was not commented on. Electromyography (EMG) studies confirmed a CFN mononeuropathy. She underwent orthopedic surgery for ligament repair 2 weeks post-injury followed by consultation with a peripheral nerve surgeon.
The patient was seen in our musculoskeletal medicine clinic for preoperative ultrasonographic assessment. She had regained partial sensation of the left distal extremity, however, remained unable to dorsiflex and evert the foot. Ultrasonographic analysis (Samsung RS80A machine, linear L4-18B probe; Samsung, Seoul, Korea) identified a tortuous fibular nerve extending 5 cm proximal to its passage over the fibular neck (Fig. 1, Supplementary Video 1). Loss of fascicular pattern began prior to division from the sciatic nerve and extended 7 cm distally, with maximal edema at 9 cm proximal to the fibular neck measuring 1 cm in diameter, with no nerve discontinuity. Common and superficial fibular nerves were unremarkable distal to the fibular neck. Upon surgical exploration, the CFN distal to its branching off the sciatic nerve was scarred and hardened. The neuroma in continuity was excised followed by grafting using cable grafts from the sural nerve. Pathology results confirmed a traumatic neuroma. At the 1-year follow-up, there was slight improvement on clinical and EMG exam in the fibular muscles (Medical Research Council Scale for Muscle Strength score 2/5), but no improvement in the muscles of the anterior compartment of the leg (tibialis anterior, extensor digitorum longus, extensor hallucis longus: strength 0/5).
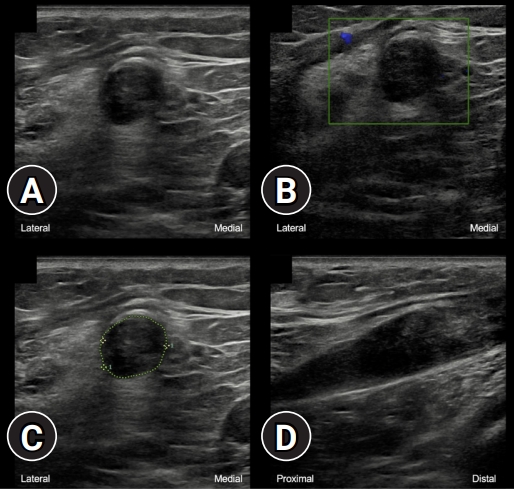
Ultrasonography of the left common fibular nerve shows intraneural swelling and loss of fascicular pattern without discontinuity after a knee posterior dislocation, in transverse axis (A) without and (B) with color doppler imaging, (C) with area (75 mm2) and diameter (9.9 mm) measurements, and (D) in longitudinal axis.
Like seven of the eight patients described by Coraci et al. [1], we did not observe CFN neurotmesis. In our patient, we additionally described distinct features of a neuroma which was tortuous at the popliteal fossa. Ultrasonographic analysis changed the course of treatment and the surgical approach. Numerous studies have shown the incidence of CFN palsy post-knee dislocation ranges from 10% to 40% [2]. Imaging findings include perineural edema, nerve discontinuity, and neuroma formation. Morris et al. [3] described a case of fibular nerve looping at the site of injury, which they termed the “lariat sign.” What we have described here is a redundant nerve in the absence of rupture, raising the question as to whether the anomaly is that of severe nerve stretching without rupture or rather nerve entrapment within disorganized fibrous scar tissue leading to its tortuous nature.
Supplementary material
Supplementary Video 1 can be found via https://doi.org/10.12701/yujm.2021.01389.
Notes
Ethical statements
Written patient consent was obtained.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Author contributions
Conceptualization: all authors; Writing-original draft: NB, MBR; Writing-review & editing, Validation: all authors.