E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(Suppl); 2023 > Article
-
Original article
Analysis of single nucleotide polymorphisms associated with the vitamin D pathway in the placentas of women with gestational diabetes mellitus: a laboratory study -
Mi Ju Kim
 , Hyun Mi Kim, Hyun-Hwa Cha, Won Joon Seong
, Hyun Mi Kim, Hyun-Hwa Cha, Won Joon Seong -
Journal of Yeungnam Medical Science 2023;40(Suppl):S9-S16.
DOI: https://doi.org/10.12701/jyms.2023.00150
Published online: May 8, 2023
Department of Obstetrics and Gynecology, Kyungpook National University Hospital, School of Medicine, Kyungpook National University, Daegu, Korea
- Corresponding author: Won Joon Seong, MD, PhD Department of Obstetrics and Gynecology, Kyungpook National University Hospital, School of Medicine, Kyungpook National University, 130 Dongdeok-ro, Jung-gu, Daegu 41944, Korea Tel: +82-53-200-5724 • Fax: +82-53-423-7905 • E-mail: wjseong@knu.ac.kr
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,229 Views
- 55 Download
Abstract
-
Background
- The aim of this study was to analyze the single nucleotide polymorphisms (SNPs) of genes known to be involved in vitamin D metabolism in the placenta using the placental tissue of mothers diagnosed with gestational diabetes mellitus (GDM) to determine whether the SNPs and occurrence of GDM are related.
-
Methods
- We enrolled 80 women of the same gestational age, 40 with and 40 without GDM. The placenta was obtained from each woman after delivery and SNP genotyping was performed on seven SNPs in the CYP27B1 (rs10877012), CYP24A1 (rs2248359, rs6013897, and rs2209314), and GC (rs2282679, rs16847024, and rs3733359) genes. Maternal serum 25-hydroxyvitamin D levels were measured during the first trimester of pregnancy and before delivery.
-
Results
- At the time of delivery, vitamin D levels were lower (21.05±12.05 mg/dL vs. 31.31±20.72 mg/dL, p=0.012) and the frequency of vitamin D deficiency was higher (60.7% vs. 32.5%, p=0.040) in the GDM group. In women with GDM, the G allele of rs10877012 was more common (86.3% vs. 65.0%, p=0.002). The rs10877012 GG genotype was more common in the GDM group (72.5% vs. 42.5%, p=0.007) and the rs10877012 TT genotype was more common in the control group (12.5% vs. 0%, p=0.007).
-
Conclusion
- Mothers with GDM have lower serum concentrations of vitamin D before delivery than healthy controls and vitamin D deficiency is common. A polymorphism in CYP27B1 (rs10877012), is considered to be a cause of GDM pathogenesis.
- Gestational diabetes mellitus (GDM) affects 1% to 14% of all pregnancies [1] and is defined as a state of glucose intolerance that occurs during pregnancy [2]. Recently, GDM has become more common due to advanced maternal age, obesity, and multiple pregnancies from the use of assisted reproductive techniques [3,4]. The occurrence of GDM and the genetic background of the patient are known to be associated because there is often a family history of GDM, and recurrence of GDM is common in subsequent pregnancies [4].
- Several factors play a role in the occurrence of GDM, and GDM has been linked to vitamin D deficiency [5]. Vitamin D is an important factor in bone metabolism and is known to cause pregnancy-related complications because of its role in pregnancy maintenance. The concentration of vitamin D in maternal blood increases throughout pregnancy, reaching approximately twice the prepregnancy concentration in the third trimester [6-8]. Moreover, the placenta regulates the expression of enzymes involved in vitamin D metabolism and the concentration of vitamin D is elevated by CYP2B1 expression, and downregulation of CYP24A1 and group-specific component, the latter of which is the main protein responsible for the transport of active vitamin D [9]. Examining the genetic variations in vitamin D pathway-regulating genes present in the placental tissue of mothers with GDM will also help us understand the genetic background of GDM.
- Single nucleotide polymorphisms (SNPs) are site-specific genome variants in which one nucleotide base is replaced with another [10]. Polymorphisms refer to mutations that occur in more than 1% of the population, while those occurring in less than 1% of the population are called mutations [11]. SNPs are the most common genetic variants and are widely used as markers for genetic mapping because of their low variability and high intergenerational stability [12,13].
- Therefore, this study analyzed the SNPs of genes known to be involved in vitamin D metabolism in the placenta using the placental tissue of mothers diagnosed with GDM to determine whether specific SNPs and the occurrence of GDM are related.
Introduction
- Ethical statements: Ethical statements: Before enrolment in the study, all participants provided informed consent. This study was approved by the Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital, Daegu, Korea (IRB No: 2018-01-010-001).
- 1. Participants and tissue sampling
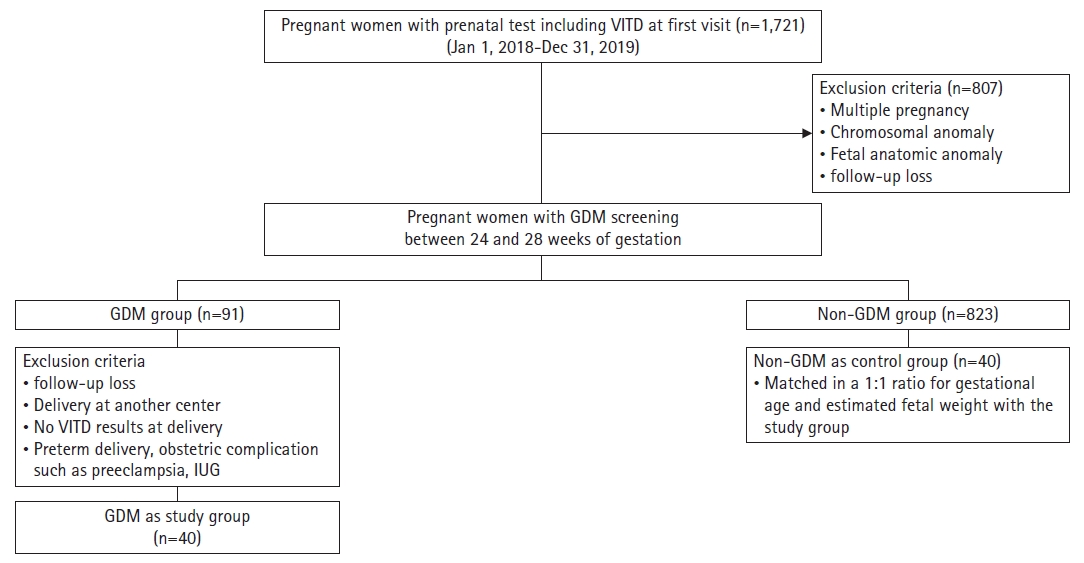
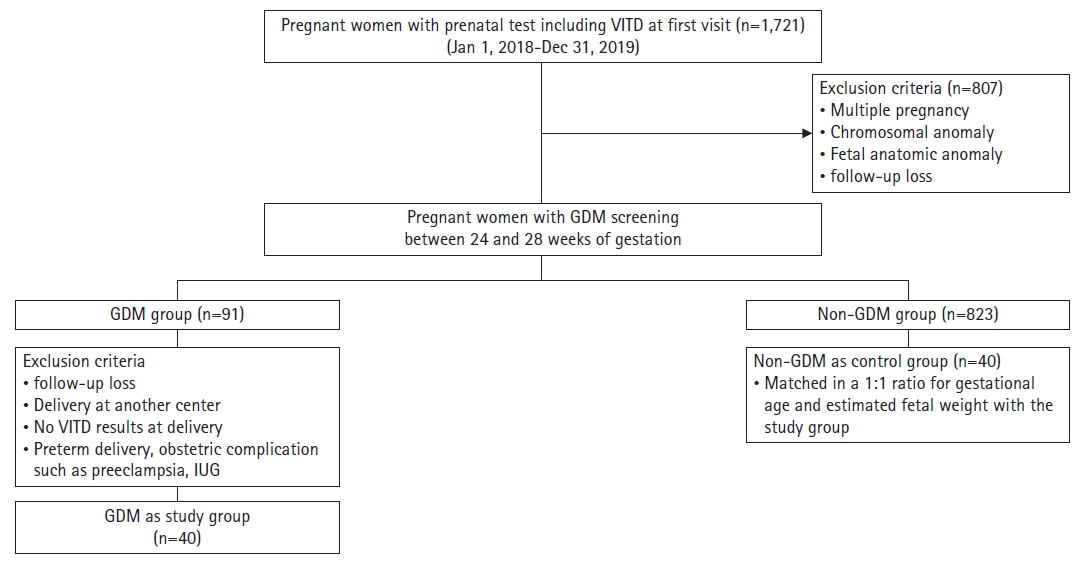
- We enrolled 40 women with GDM and 40 women without GDM of the same gestational age as the control group. GDM was diagnosed using a two-step approach: a 50-g glucose tolerance test as a screening test between 24 and 28 weeks of gestation and a 100-g glucose tolerance test when the initial test value was greater than 140 mg/dL. In addition, the Carpenter–Coustan criteria were used to diagnose GDM [14]. All women delivered at full term and had no fetal chromosomal or structural anomalies. Women with pregnancy-related complications or risk factors, such as multiple pregnancies, gestational hypertension, preeclampsia, preterm labor, and fetal growth restriction, were excluded from this study (Fig. 1). Maternal blood was drawn from a cannulated vein during the first trimester of pregnancy and before delivery, and 25-hydroxyvitamin D (25(OH)D) levels were determined using a commercial enzyme immunoassay kit. A level of 25(OH)D <20 mg/dL was defined as vitamin D deficiency [15,16]. For all 80 participants, the placenta was cut into 1×1-cm pieces and stored in a freezer at –70°C immediately after delivery.
- 2. Single nucleotide polymorphism selection
- SNP genotyping was performed on seven SNPs in CYP27B1 (rs10877012), CYP24A1 (rs2248359, rs6013897, and rs2209314), and GC (rs2282679, rs16847024, and rs3733359). In this study, a minor allele frequency (MAF) of ≥0.05 was used to filter SNPs that are published in the NCBI Variation Viewer (https://www.ncbi.nlm.nih.gov/variation/view/). The SNPs were selected based on their potential biological significance.
- 3. DNA extraction and genotyping
- The QIAamp Fast DNA Tissue Kit (Qiagen, Valencia, CA, USA) was used to extract genomic DNA from the postoperative placental tissue, and the quality and quantity of the extracted DNA were evaluated using a NanoDrop ND-2000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA) [17].
- SNP genotyping was performed on an Applied Biosystems 7500 real-time polymerase chain reaction (PCR) system (Applied Biosystems, Foster City, CA, USA) using rhAmp SNP Assays (Integrated DNA Technologies, Coralville, IA, USA) and TaqMan SNP Genotyping Assays (Applied Biosystems). Table 1 lists the predesigned assays.
- The rhAmp SNP Genotyping Assay was performed in accordance with the manufacturer’s instructions. The 10-μL PCR mix included 5 ng of DNA, 5.3 μL of Combined Master Mix and Reporter Mix, 2× rhAmp Genotyping Master Mix (Integrated DNA Technologies), 40× rhAmp Reporter Mix with Reference (Integrated DNA Technology), and 0.5 μL of rhAmp SNP assays (Integrated DNA Technologies). The PCR cycling was performed according to the manufacturer’s recommendation (60°C for 1 minute, 95°C for 10 minutes, followed by 40 cycles of 95°C for 10 seconds, 60°C for 30 seconds, and 68°C for 20 seconds).
- The TaqMan SNP Genotyping Assay was performed following the manufacturer’s instructions. The 10-μL PCR mix comprised 10 ng of genomic DNA, 5.0 μL of 2× TaqMan Universal PCR Master Mix No UNG, and 0.5 μL of 20× SNP Genotyping Assay (probes and primers). The PCR cycling was performed according to the manufacturer’s recommendation (60°C for 1 minute, 95°C for 10 minutes, followed by 40 cycles of 92°C for 15 seconds and 60°C for 60 seconds).
- Using the chi-square tests, the genotype frequencies of the given data were examined for compliance with the Hardy–Weinberg equilibrium.
- 4. Statistical analysis
- Haploview software ver. 4.2 (Broad Institute, Cambridge, MA, USA; http://broadinstitute.org/haploview/haploview) was used to analyze linkage disequilibrium (LD). LD patterns were created using an algorithm designed by Gabriel et al. [17] with a MAF of ≥1%.
- The Hardy–Weinberg equilibrium and chi-square tests were used to compare variables between the two groups [18] using IBM SPSS ver. 26 (IBM Corp., Armonk, NY, USA). A two-sided p-value of <0.05 was considered statistically significant.
Methods
- Table 2 summarizes the baseline characteristics of patients in the GDM and control groups. There were no significant differences between the two groups in terms of gestational age at delivery, birth weight, or placental weight. However, the maternal age, prepregnancy maternal weight, and body mass index (BMI) were higher in the GDM group than in the control group. At the time of delivery, vitamin D levels were lower (21.05±12.05 mg/dL vs. 31.31±20.72 mg/dL, p=0.012) and the frequency of vitamin D deficiency was higher (60.7% vs. 32.5%, p=0.040) in the GDM group than in the control group. To determine whether significant differences in maternal age and prepregnancy BMI between the GDM and control groups affected vitamin D levels, these confounding factors were corrected and analyzed. The results also confirmed that vitamin D levels in the GDM group were lower than those in the control group.
- All observed allele and genotype frequencies were in Hardy–Weinberg equilibrium. Table 3 shows that there was no statistically significant difference in the allele frequencies of all SNPs except for rs10877012. In women with GDM, the G allele of rs10877012 was more common (86.3% vs. 65.0%, p=0.002). In addition, the allele frequency of rs2248359 showed borderline significance (p=0.051). Table 4 shows the genotype frequencies of the SNPs. Among the seven SNPs studied, rs10877012 revealed the most significant difference, with the rs10877012 GG genotype being more common in the GDM group (72.5% vs. 42.5%, p=0.007) and the rs10877012 TT genotype being more common in the control group (0% vs. 12.5%, p=0.007). Although not statistically significant, the rs6013897 TT genotype was less common in the GDM group (p=0.051).
Results
- Vitamin D is a steroid hormone responsible for the metabolism of calcium and phosphorus and is associated with bone mineralization; however, it is also linked to the pathogenesis of various diseases. In particular, it has been reported to be closely related to cardiovascular disease [19], cancerous conditions such as colorectal cancer [20], obesity [15], and autoimmunity [21]. In the field of obstetrics, vitamin D is associated with preterm birth [22] and preeclampsia [23,24]. In addition, it acts on beta cells, affecting GDM occurrence [25], implying that genetic variation in the vitamin D pathway is a major risk factor for GDM.
- In general, vitamin D concentration is regulated by the activity of enzymes found in the kidneys. 1-Hydroxylase (i.e., CYP27B1) converts 25(OH)D into 1,25-dihydroxyvitamin D (1,25(OH)2D), an active form with biological functions, whereas 24-hydroxylase (i.e., CYP24A1) catabolizes 25(OH)D and 1,25(OH)2D into inactive forms. 25(OH)D is the main circulating metabolite of vitamin D and is an indicator of vitamin D concentration [15]. During pregnancy, 1-hydroxylase, 24-hydroxylase, vitamin D receptor, and vitamin D-binding protein are found in the placenta, indicating that the placenta is closely involved in vitamin D metabolism [24,26,27].
- In this study, mothers with GDM had lower serum vitamin D concentrations before delivery and a higher incidence of vitamin D deficiency than those in the control group. The GDM group was older than the control group and had a higher BMI before pregnancy. However, after correcting for confounding factors, the GDM group also had lower vitamin D levels. Agüero-Domenech et al. [28] reported in 2021 on the relationship between vitamin D, GDM, and BMI, indicating that vitamin D levels and BMI were not significantly related in patients with GDM. In the present study, there was no statistically significant difference between the GDM and control groups with respect to vitamin D supplementation. Vitamin D levels were not significantly different in the two groups in the first trimester of pregnancy but were significantly different just before delivery. Thus, vitamin D may have a certain effect on GDM pathogenesis and metabolism.
- Consistent with this study, several papers have already reported that GDM and vitamin D deficiency measured in the third trimester of pregnancy are closely related [16,29,30]. A previous study showed that lower vitamin D levels measured at 16 weeks of gestation increased the risk of future GDM [29]; however, another study found no link between vitamin D deficiency and GDM in the first trimester of pregnancy [31]. In the present study, vitamin D concentration in the first trimester of pregnancy was slightly higher in the GDM group than in the control group; however, the difference was not statistically significant, confirming the above findings. Vitamin D is produced in the placenta during pregnancy, and its concentration increases as the placental mass increases [16,32]. It can be seen that the association between GDM and vitamin D levels differs depending on the stage of pregnancy.
- Cho et al. [16] reported an increase in the expression of CYP24A1, which is involved in the vitamin D pathway, in the placentas of mothers with GDM and found a link between its expression and blood vitamin D levels. Zhou et al. [33] studied the association between GDM occurrence and vitamin D receptor gene polymorphisms. In the present study, no statistically significance difference in CYP24A1 coding SNPs was found, but the difference between SNPs encoding the CYP27B1 gene was confirmed. In women with GDM, the rs10877012 G allele was the most common. Furthermore, the rs10877012 GG genotype was more common in the GDM group, whereas the rs10877012 TT genotype was more common in the control group. CYP27B1 is located on 12q14.1 and is composed of nine exons [20]. The rs10877012 is located in the CYP27B1 promoter, plays an important role in transcription and translation, and is related to the concentration of circulating 25(OH)D [34]. According to the SNP database, the MAF was found to be 27.8% in the global population, 35.0% in the control group, and 13.75% in the GDM group in this study.
- The CYP27B1 gene polymorphism rs10877012 is associated with the development and prognosis of various diseases such as colorectal cancer, asthma, and chronic hepatitis C [20,35,36]. Moreover, a recent meta-analysis suggested that this CTP27B1 gene polymorphism is related to susceptibility to organ-specific autoimmune endocrine diseases [37]. Several studies have attempted to determine the correlation between type 1 diabetes mellitus (not GDM) and CYP27B1 gene polymorphisms but have not obtained consistent results [38-40].
- The strength of the present study is that, to the best of our knowledge, it is the first to show a link between the CYP27B1 rs10877012 polymorphism and the occurrence of GDM, and the first to compare vitamin D levels in the first trimester of pregnancy and just before delivery in GDM and control groups. However, a limitation of this study is the small sample size. Both rs2248359 and rs6013897 polymorphisms showed borderline significance, emphasizing the need for further large-sample studies. GDM is caused by a complex mechanism and combination of various factors. In this study, a CYP27B1 gene polymorphism involved in the vitamin D pathway was identified, and its association with gestational diabetes was considered. We do not think that this one factor is the only mechanism underlying the disease. Furthermore, a long-term follow-up study will be needed in the future, and it will be interesting to learn about the differences in SNPs between the two groups, especially when mothers with GDM develop overt diabetes mellitus in the future versus those who do not.
- In summary, mothers with GDM have lower serum concentrations of vitamin D before delivery than healthy controls, and vitamin D deficiency is common. This may be due to polymorphisms in a gene involved in vitamin D metabolism in the placenta. The CYP27B1 polymorphism of the CYP27B1 gene rs10877012 can also be considered one of the various causes of GDM pathogenesis.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This research was supported by the Kyungpook National University Research Fund, 2021.
-
Author contributions
Conceptualization: All authors; Investigation, Data curation: MJK, HMK, HHC; Formal analysis: HMK, HHC, WJS; Funding acquisition: MJK; Supervision: WJS; Writing-original draft: MJK; Writing-review & editing: WJS.
Notes
| Characteristic | GDM group (n=40) | Control group (n=40) | p-value |
|---|---|---|---|
| Age (yr) | 35.21±3.43 | 32.95±4.24 | 0.011a) |
| Nullipara (%) | 41.0 | 47.50 | 0.724 |
| Height (cm) | 160.42 ±5.14 | 161.20 ±4.43 | 0.474 |
| Prepregnancy body weight (kg) | 64.77±14.52 | 58.33±9.45 | 0.023a) |
| Delivery maternal body weight (kg) | 73.80±13.81 | 69.70±9.83 | 0.133 |
| Prepregnancy BMI (kg/m2) | 25.28±5.55 | 22.48±3.83 | 0.012a) |
| Vitamin D level at 1st trimester (mg/dL) | 13.73±5.04 | 19.06±12.67 | 0.102 |
| Vitamin D deficiency at 1st trimester (%) | 83.3 | 77.273 | 0.937 |
| Vitamin D level at delivery (mg/dL) | 21.05±12.05 | 31.31±20.72 | 0.012a) |
| Vitamin D deficiency at delivery (%) | 60.7 | 32.5 | 0.040a) |
| Gestational age at delivery (wk) | 38.14±0.87 | 38.51±1.16 | 0.123 |
| Birthweight (g) | 3,089.00±474.91 | 3,113.50±434.05 | 0.815 |
| Male sex (%) | 46.2 | 42.50 | 0.920 |
| Placental weight (g) | 684.36±138.12 | 668.00±117.76 | 0.572 |
| Total calcium level (mg/dL) | 10.01±0.58 | 9.61±0.66 | 0.422 |
| Phosphate level (mg/dL) | 5.09±0.61 | 5.47±1.20 | 0.230 |
| SNP | GDM group | Control group | p-value |
|---|---|---|---|
| rs10877012 | 0.002a) | ||
| G | 69 (86.3) | 52 (65.0) | |
| T | 11 (13.8) | 28 (35.0) | |
| rs2248359 | 0.051 | ||
| C | 43 (53.8) | 55 (68.8) | |
| T | 37 (46.3) | 25 (31.3) | |
| rs6013897 | 0.077 | ||
| T | 64 (80.0) | 72 (90.0) | |
| A | 16 (20.0) | 8 (10.0) | |
| rs2209314 | 0.521 | ||
| T | 45 (56.3) | 49 (61.3) | |
| C | 35 (43.8) | 31 (38.8) | |
| rs2282679 | 0.235 | ||
| T | 51 (63.8) | 58 (72.5) | |
| G | 29 (36.3) | 22 (27.5) | |
| rs16847024 | 0.807 | ||
| C | 71 (88.8) | 70 (87.5) | |
| T | 9 (11.3) | 10 (12.5) | |
| rs3733359 | 0.603 | ||
| G | 55 (68.8) | 58 (72.5) | |
| A | 25 (31.3) | 22 (17.5) |
| SNP | GDM group | Control group | p-value |
|---|---|---|---|
| rs10877012 | 0.007a) | ||
| G/G | 29 (72.5) | 17 (42.5) | |
| G/T | 11 (27.5) | 18 (45.0) | |
| T/T | 0 (0) | 5 (12.5) | |
| rs2248359 | 0.090 | ||
| C/C | 9 (22.5) | 18 (45.0) | |
| C/T | 25 (62.5) | 19 (47.5) | |
| T/T | 6 (15.0) | 3 (7.5) | |
| rs6013897 | 0.051 | ||
| T/T | 24 (60.0) | 32 (75.0) | |
| T/A | 16 (40.0) | 8 (25.0) | |
| A/A | 0 (0) | 0 (0) | |
| rs2209314 | 0.458 | ||
| T/T | 14 (35.0) | 14 (35.0) | |
| T/C | 17 (42.5) | 21 (52.5) | |
| C/C | 9 (22.5) | 5 (12.5) | |
| rs2282679 | 0.415 | ||
| T/T | 16 (40.0) | 20 (50.0) | |
| T/G | 19 (47.5) | 18 (45.0) | |
| G/G | 5 (12.5) | 2 (5.0) | |
| rs16847024 | 0.960 | ||
| C/C | 32 (80.0) | 31 (77.5) | |
| C/T | 7 (17.5) | 8 (20.0) | |
| T/T | 1 (2.5) | 1 (2.5) | |
| rs3733359 | 0.872 | ||
| G/G | 19 (47.5) | 21 (52.5) | |
| G/A | 17 (42.5) | 16 (40.0) | |
| A/A | 4 (10.0) | 3 (7.5) |
- 1. Bener A, Saleh NM, Al-Hamaq A. Prevalence of gestational diabetes and associated maternal and neonatal complications in a fast-developing community: global comparisons. Int J Womens Health 2011;3:367–73.ArticlePubMedPMC
- 2. Reece EA, Leguizamón G, Wiznitzer A. Gestational diabetes: the need for a common ground. Lancet 2009;373:1789–97.ArticlePubMed
- 3. Schwartz N, Nachum Z, Green MS. The prevalence of gestational diabetes mellitus recurrence: effect of ethnicity and parity: a metaanalysis. Am J Obstet Gynecol 2015;213:310–7.ArticlePubMed
- 4. Kim C, Berger DK, Chamany S. Recurrence of gestational diabetes mellitus: a systematic review. Diabetes Care 2007;30:1314–9.ArticlePubMed
- 5. Wen L, Liu X, Wang L, Zheng Y, Li J, Tong C, et al. Correlation between second trimester weight gain and perinatal outcomes in dichorionic twin pregnancies: the LoTiS cohort study. Eur J Obstet Gynecol Reprod Biol 2019;233:64–9.ArticlePubMed
- 6. Cross NA, Hillman LS, Allen SH, Krause GF, Vieira NE. Calcium homeostasis and bone metabolism during pregnancy, lactation, and postweaning: a longitudinal study. Am J Clin Nutr 1995;61:514–23.ArticlePubMed
- 7. Ritchie LD, Fung EB, Halloran BP, Turnlund JR, Van Loan MD, Cann CE, et al. A longitudinal study of calcium homeostasis during human pregnancy and lactation and after resumption of menses. Am J Clin Nutr 1998;67:693–701.ArticlePubMed
- 8. Shin JS, Choi MY, Longtine MS, Nelson DM. Vitamin D effects on pregnancy and the placenta. Placenta 2010;31:1027–34.ArticlePubMedPMC
- 9. Saffery R, Ellis J, Morley R. A convergent model for placental dysfunction encompassing combined sub-optimal one-carbon donor and vitamin D bioavailability. Med Hypotheses 2009;73:1023–8.ArticlePubMed
- 10. Venter JC, Adams MD, Myers EW, Li PW, Mural RJ, Sutton GG, et al. The sequence of the human genome. Science 2001;291:1304–51.ArticlePubMed
- 11. Wang DG, Fan JB, Siao CJ, Berno A, Young P, Sapolsky R, et al. Large-scale identification, mapping, and genotyping of single-nucleotide polymorphisms in the human genome. Science 1998;280:1077–82.ArticlePubMed
- 12. Conrad DF, Jakobsson M, Coop G, Wen X, Wall JD, Rosenberg NA, et al. A worldwide survey of haplotype variation and linkage disequilibrium in the human genome. Nat Genet 2006;38:1251–60.ArticlePubMedPDF
- 13. Ardlie KG, Kruglyak L, Seielstad M. Patterns of linkage disequilibrium in the human genome. Nat Rev Genet 2002;3:299–309.ArticlePubMedPDF
- 14. Carpenter MW, Coustan DR. Criteria for screening tests for gestational diabetes. Am J Obstet Gynecol 1982;144:768–73.ArticlePubMed
- 15. Yu S, Feng Y, Qu C, Huo W, Mao Z, Wang C, et al. CYP27B1 as an instrument gene to investigate the causal relationship between vitamin D deficiency and obesity: a family-based study. Eur J Clin Nutr 2020;74:806–10.ArticlePubMedPDF
- 16. Cho GJ, Hong SC, Oh MJ, Kim HJ. Vitamin D deficiency in gestational diabetes mellitus and the role of the placenta. Am J Obstet Gynecol 2013;209:560.Article
- 17. Gabriel SB, Schaffner SF, Nguyen H, Moore JM, Roy J, Blumenstiel B, et al. The structure of haplotype blocks in the human genome. Science 2002;296:2225–9.ArticlePubMed
- 18. Rodriguez S, Gaunt TR, Day IN. Hardy-Weinberg equilibrium testing of biological ascertainment for Mendelian randomization studies. Am J Epidemiol 2009;169:505–14.ArticlePubMedPMC
- 19. Pilz S, Verheyen N, Grübler MR, Tomaschitz A, März W. Vitamin D and cardiovascular disease prevention. Nat Rev Cardiol 2016;13:404–17.ArticlePubMedPDF
- 20. Latacz M, Snarska J, Kostyra E, Wroński K, Fiedorowicz E, Savelkoul H, et al. CYP27B1 gene polymorphism rs10877012 in patients diagnosed with colorectal cancer. Nutrients 2020;12:998.ArticlePubMedPMC
- 21. Ruiz-Ballesteros AI, Meza-Meza MR, Vizmanos-Lamotte B, Parra-Rojas I, de la Cruz-Mosso U. Association of vitamin D metabolism gene polymorphisms with autoimmunity: evidence in population genetic studies. Int J Mol Sci 2020;21:9626.ArticlePubMedPMC
- 22. Manzon L, Altarescu G, Tevet A, Schimmel MS, Elstein D, Samueloff A, et al. Vitamin D receptor polymorphism FokI is associated with spontaneous idiopathic preterm birth in an Israeli population. Eur J Obstet Gynecol Reprod Biol 2014;177:84–8.ArticlePubMed
- 23. Bodnar LM, Simhan HN, Catov JM, Roberts JM, Platt RW, Diesel JC, et al. Maternal vitamin D status and the risk of mild and severe preeclampsia. Epidemiology 2014;25:207–14.ArticlePubMedPMC
- 24. Lechtermann C, Hauffa BP, Herrmann R, Schündeln MM, Gellhaus A, Schmidt M, et al. Maternal vitamin D status in preeclampsia: seasonal changes are not influenced by placental gene expression of vitamin D metabolizing enzymes. PLoS One 2014;9:e105558.ArticlePubMedPMC
- 25. Joergensen JS, Lamont RF, Torloni MR. Vitamin D and gestational diabetes: an update. Curr Opin Clin Nutr Metab Care 2014;17:360–7.ArticlePubMed
- 26. Díaz L, Arranz C, Avila E, Halhali A, Vilchis F, Larrea F. Expression and activity of 25-hydroxyvitamin D-1 alpha-hydroxylase are restricted in cultures of human syncytiotrophoblast cells from preeclamptic pregnancies. J Clin Endocrinol Metab 2002;87:3876–82.ArticlePubMed
- 27. Ma R, Gu Y, Zhao S, Sun J, Groome LJ, Wang Y. Expressions of vitamin D metabolic components VDBP, CYP2R1, CYP27B1, CYP24A1, and VDR in placentas from normal and preeclamptic pregnancies. Am J Physiol Endocrinol Metab 2012;303:E928–35.ArticlePubMedPMC
- 28. Agüero-Domenech N, Jover S, Sarrión A, Baranda J, Quesada-Rico JA, Pereira-Expósito A, et al. Vitamin D deficiency and gestational diabetes mellitus in relation to body mass index. Nutrients 2021;14:102.ArticlePubMedPMC
- 29. Zhang C, Qiu C, Hu FB, David RM, van Dam RM, Bralley A, et al. Maternal plasma 25-hydroxyvitamin D concentrations and the risk for gestational diabetes mellitus. PLoS One 2008;3:e3753.ArticlePubMedPMC
- 30. Maghbooli Z, Hossein-Nezhad A, Karimi F, Shafaei AR, Larijani B. Correlation between vitamin D3 deficiency and insulin resistance in pregnancy. Diabetes Metab Res Rev 2008;24:27–32.ArticlePubMed
- 31. Baker AM, Haeri S, Camargo CA Jr, Stuebe AM, Boggess KA. First-trimester maternal vitamin D status and risk for gestational diabetes (GDM) a nested case-control study. Diabetes Metab Res Rev 2012;28:164–8.ArticlePubMedPMC
- 32. Delvin EE, Arabian A. Kinetics and regulation of 25-hydroxycholecalciferol 1 alpha-hydroxylase from cells isolated from human term decidua. Eur J Biochem 1987;163:659–62.ArticlePubMed
- 33. Zhou Q, Wen S, Liu M, Zhang S, Jin X, Liu A. Association between gene polymorphisms of vitamin D receptor and gestational diabetes mellitus: a systematic review and meta-analysis. Int J Environ Res Public Health 2020;18:205.ArticlePubMedPMC
- 34. Signorello LB, Shi J, Cai Q, Zheng W, Williams SM, Long J, et al. Common variation in vitamin D pathway genes predicts circulating 25-hydroxyvitamin D levels among African Americans. PLoS One 2011;6:e28623.ArticlePubMedPMC
- 35. Lahmar O, Salhi M, Kaabachi W, Berraies A, Ammar J, Soomro MH, et al. Association between vitamin D metabolism gene polymorphisms and risk of Tunisian adults’ asthma. Lung 2018;196:285–95.ArticlePubMedPDF
- 36. Lange CM, Bibert S, Kutalik Z, Burgisser P, Cerny A, Dufour JF, et al. A genetic validation study reveals a role of vitamin D metabolism in the response to interferon-alfa-based therapy of chronic hepatitis C. PLoS One 2012;7:e40159.ArticlePubMedPMC
- 37. Ma X, Xie Z, Qin J, Luo S, Zhou Z. Association of vitamin D pathway gene CYP27B1 and CYP2R1 polymorphisms with autoimmune endocrine disorders: a meta-analysis. J Clin Endocrinol Metab 2020;105:3575–87.ArticlePubMedPDF
- 38. Bailey R, Cooper JD, Zeitels L, Smyth DJ, Yang JH, Walker NM, et al. Association of the vitamin D metabolism gene CYP27B1 with type 1 diabetes. Diabetes 2007;56:2616–21.ArticlePubMedPDF
- 39. Nam HK, Rhie YJ, Lee KH. Vitamin D level and gene polymorphisms in Korean children with type 1 diabetes. Pediatr Diabetes 2019;20:750–8.ArticlePubMedPDF
- 40. Hussein AG, Mohamed RH, Alghobashy AA. Synergism of CYP2R1 and CYP27B1 polymorphisms and susceptibility to type 1 diabetes in Egyptian children. Cell Immunol 2012;279:42–5.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite