Dynamic ultrasound examination of the median nerve during follow-up after wrist fracture/surgery
Article information

Owing to its advantages, ultrasound examination of peripheral nerve injuries is paramount [1]. Herein, we present two cases of median nerve entrapment after internal fixation surgery for fractures of the wrist, one of the carpal bones, and the other of the distal radius.
A 51-year-old female presented with numbness/tingling of the thumb and index finger of her right hand. Her complaints ensued after a fracture of the carpal bones (and subsequent internal fixation surgery) 6 years prior. Her medical history was unremarkable. Ultrasonography revealed a mild swelling of the right median nerve, which was located close to the fixation material (Fig. 1). The median nerve was further impinged during wrist movements. During wrist extension/flexion, compression of the median nerve and the patient’s symptoms became more apparent (Supplementary Video 1). Accordingly, the median nerve pathology was directly attributed to the internal fixation material. The results of previous electrodiagnostic evaluations were unremarkable. As the patient refused secondary corrective surgery, she was provided wrist splints and analgesics.
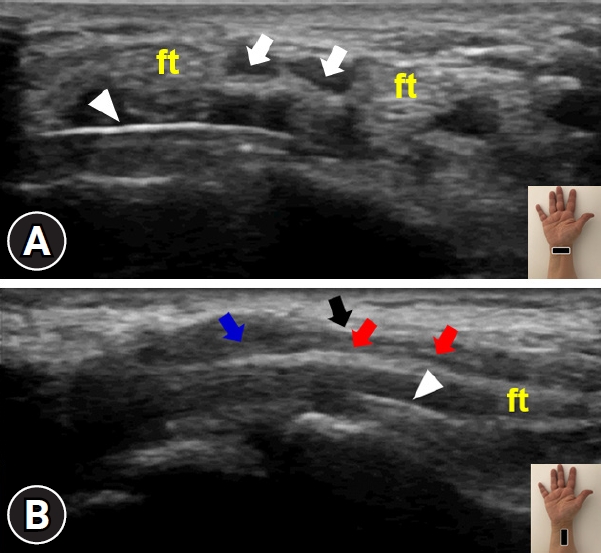
Ultrasound imaging of the median nerve at the volar wrist. (A) Short-axis view depicts the close relationship between the bifid median nerve (white arrows) and the metal plate (arrowheads). (B) Long-axis view clearly shows the swollen median nerve (red vs. blue arrows) distal to compression (black arrow) by the underlying metal plate (arrowhead). Insets show the transducer’s position. ft, flexor tendon.
The second case involved a 54-year-old female with fractures of the distal radius and ulnar styloid process. She wore a cast for 5 weeks and then underwent internal fixation of the distal radius (Fig. 2). She later complained of pain/dysesthesia in the first three fingers of the right hand. Upon ultrasound examination, the median nerve and metallic plate were located close to each other on both short- and long-axis imaging (Supplementary Fig. 1). On dynamic ultrasound examination (Supplementary Videos 2, 3), the median nerve appeared to be very close to and intermittently irritated by the underlying metallic plate on the distal radius. The median nerve was much more compressed during wrist flexion/extension movements. Furthermore, the patient described pain/dysesthesia during the dynamic, real-time ultrasound examination. Again, the metallic plate was thought to be the direct cause of median nerve irritation. The patient had not undergone electrodiagnostic testing before. She was prescribed physical therapy (whirlpool and exercise).

Anteroposterior radiograph shows the metal plate in the radius and the fracture of the ulnar styloid (arrowhead).
Median neuropathy can be observed after wrist fractures are treated with internal fixation [2]. In a cohort of 2,908 patients, distal radius fractures treated with open reduction and internal fixation surgery were associated with postoperative carpal tunnel syndrome [3]. In most relevant cases, diagnosis and follow-up were performed using physical and electrophysiological examinations. In this sense, calling attention to its numerous advantages—for example, patient/physician-friendly, convenient, radiation-free, and allowing dynamic evaluation—we highlight the paramount role of ultrasound examination in the prompt management of these cases. When ultrasound waves encounter highly reflective or absorbing surfaces such as bone, calcification, or metal plates, a hypoechoic area appears below the surface. This type of artifact is known as posterior acoustic shadowing [4]. One of the most important advantages of ultrasound is that it allows dynamic assessment of median nerve mobility [5]. Confirming the entrapment of the nerve(s) using different maneuvers, as well as sono-Tinel, cannot be performed with other imaging modalities, especially when the surgical materials are not compatible with imaging.
Notes
Ethical statements
Informed patient consent was obtained from both patients included in the study.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Supplementary materials
Supplementary Fig. 1 and Supplementary Videos 1¬–3 can be found at https://doi.org/10.12701/jyms.2023.01291.
Ultrasound imaging of the median nerve at the volar wrist. (A) Short-axis and (B) long-axis views show the median nerve (arrowheads) and metallic plate (arrows), which are located close to each other. Insets show the transducer’s position.
(Longitudinal view) Dynamic ultrasound imaging of the right volar wrist. The swollen median nerve compressed by the metal plate is visualized during wrist movements.
(Axial view) Dynamic ultrasound imaging of the right volar wrist. The median nerve and metal plate are closely affected by flexion and extension of the wrist.
(Longitudinal view) Dynamic ultrasound imaging of the right volar wrist. The median nerve and metal plate are very close to each other during wrist movements.