Coinfection of Sphingomonas paucimobilis meningitis and Listeria monocytogenes bacteremia in an immunocompetent patient: a case report
Article information

Abstract
This report describes a case of coinfection of Sphingomonas paucimobilis meningitis and Listeria monocytogenes bacteremia in a 66-year-old immunocompetent female patient. The patient had undergone traditional procedures, including acupuncture, which possibly caused the coinfection. During treatment with susceptible antibiotics for bacterial meningitis, she developed hydrocephalus on the third day. Consequently, the patient recovered with a mild neurological deficit of grade 4 motor assessment in both upper and lower extremities at discharge. S. paucimobilis and L. monocytogenes are rare pathogens in developed countries, occurring only during environmental outbreaks. S. paucimobilis meningitis is rarely reported. Hence, the various presentations of S. paucimobilis meningitis and the antibiotic regimen for its treatment are hereby reported, in addition to a review of other similar reported cases. This case is a possible traditional procedure-related infection. Appropriate oversight and training should be emphasized regarding preventive measures of this kind of infection. A team approach with neurologists and neurosurgeons is imperative in treating patients with hydrocephalus-complicated meningitis.
Introduction
Sphingomonas paucimobilis is a gram-negative, nonfermenter, and community-acquired bacteria [1]. Sphingomonas spp. has been isolated from seawater, river water, wastewater, mineral water, and water-based hospital equipment [2]. Several hospital outbreaks of S. paucimobilis, mainly catheter-associated infections, have been reported [3,4]. Although S. paucimobilis has low virulence, it may still cause meningitis and bacteremia. S. paucimobilis infection involving the central nervous system can manifest as meningitis and ventriculitis.
Listeria monocytogenes is a gram-positive pathogenic bacterium found in soil and water [5]. Community-acquired infections generally occur during foodborne outbreaks [6]. Common L. monocytogenes infections have been reported as gastrointestinal tract infections, meningitis, and bacteremia [6,7]. Infections in neonates and the elderly have higher rates of mortality and morbidity [6,7].
This case report described the case of an immunocompetent host with S. paucimobilis meningitis and L. monocytogenes bacteremia.
Case
Ethical statements: This study was approved by the Institutional Review Board (IRB) of the Yeungnam University Hospital (IRB No: 2020-01-018). Written informed consent was obtained for publication of this case report and accompanying images.
A 66-year-old woman complained of fever, slight drowsiness, and neck stiffness for 5 days. The patient complained of no gastrointestinal symptoms. Eight days before her admission, she had received acupuncture more than 100 times and moxibustion cupping on both sides of her posterior neck. She had no history of diabetes, hypertension, or corticosteroid use. Thirteen months before this event, the patient had received her final adjuvant chemotherapy for breast cancer after mastectomy. One day before her admission, she had visited a nearby hospital, and the brain magnetic resonance imaging (MRI) findings were unremarkable and showed no meningeal enhancement. The hospital referred her to a tertiary hospital for further evaluation of her neck stiffness as she had no Kernig or Brudzinski signs. There were few round thin bruise-like lesions from the previous cupping procedure without tenderness or swelling on inspection. Her vital signs were as follows: blood pressure, 160/100 mmHg; heart rate, 75 beats/min; respiratory rate, 20 breaths/min; and body temperature, 39.1°C. Her initial Glasgow Coma Scale (GCS) score was 15, while her motor assessment result was grade 5. Her sensory assessment result was unremarkable. The initial cerebrospinal fluid (CSF) analysis results revealed a white blood cell (WBC) count of 429/μL (polymorphonucleocytes [PMN], 62%), red blood cell count of 100/μL, glucose of 11 mg/dL, adenosine deaminase of 19.7 IU/L, protein level of 369.51 mg/dL, and an opening pressure of 100 mmHg. The fluid was yellowish with a turbid nature. For culture, an uncentrifuged CSF sample was inoculated onto one blood agar plate (Komed Corp., Ltd., Seongnam, Korea), one chocolate agar plate (Komed Corp., Ltd.), and BBL Fluid thioglycollate medium (BD, Sparks, MD, USA). Identification and antimicrobial susceptibility tests were performed using VITEK 2 (software version 08.01; bioMérieux, Marcy-l'Étoile, France). The laboratory blood results were as follows: WBC of 11,520/μL, hemoglobin of 13 g/dL, high-sensitivity C-reactive protein of 18.791 mg/dL, erythrocyte sedimentation rate of 33 mm/hr, glucose of 174 mg/dL, and total protein of 6.08 g/L. For blood culture, each bottle of two blood culture media sets (BACT/ALERT SA & SN; bioMérieux) was inoculated with 10 to 15 mL of blood. The identification process was performed using VITEK MS (bioMérieux). VITEK 2 was used for antimicrobial susceptibility tests for the blood culture. The patient was diagnosed with bacterial meningitis. She received antibiotic treatment with vancomycin and ceftazidime. Intravenous dexamethasone sodium phosphate (0.6 mg/kg/day every 6 hours) was given for 5 days.
On her third hospitalization day (HD), her mental status deteriorated, and she was intubated. Subsequently, brain computed tomography (CT) showed signs consistent with hydrocephalus (Fig. 1), and an emergency external ventricular drainage (EVD) was inserted. On HD 5, the culture results of the initial CSF sample revealed S. paucimobilis, which was susceptible to cefotaxime (minimal inhibitory concentration [MIC] ≤1), ciprofloxacin (MIC=0.5), ceftazidime (MIC=8), and cefepime (MIC ≤1) but resistant to colistin (MIC ≥16). Two bottles of the initial blood culture results revealed L. monocytogenes susceptible to ampicillin (MIC ≤0.25) and vancomycin (MIC=0.5) but resistant to ciprofloxacin (MIC=1) and oxacillin (MIC ≥4). The treatment was switched to ampicillin/sulbactam and ceftriaxone on the HD 6.
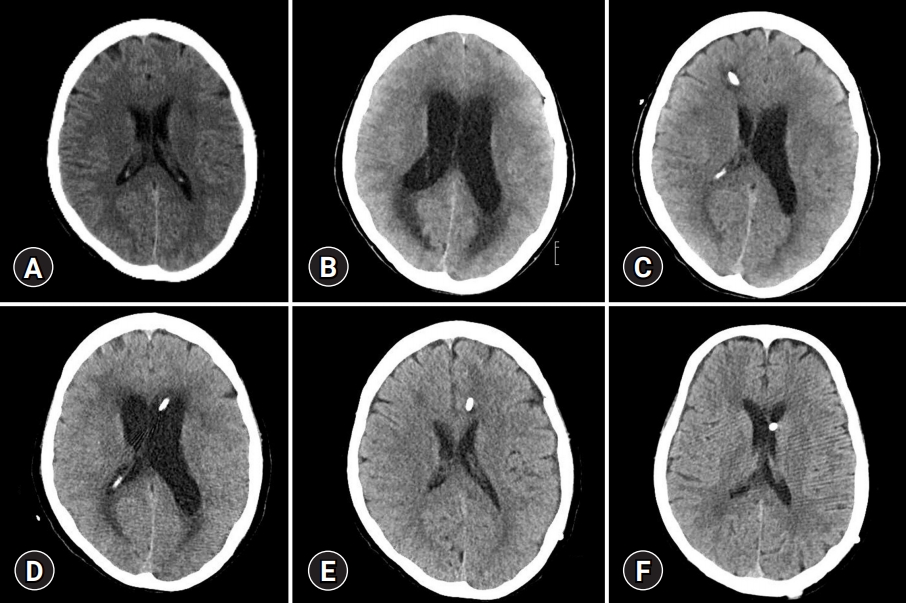
Computed tomography images of the brain. (A) On hospitalization day (HD) 1, without enlarged ventricles; (B) on HD 3, with the enlarged ventricle; (C) on HD 10, with the enlarged left ventricle and emergency external ventricular drainage, inserted at right Kocher's point; (D) on HD 32, with the enlarged ventricle and emergency external ventricular drainage, inserted at left Kocher's point; (E) on HD 45, with a normal ventricle size and ventriculoperitoneal (VP) shunt inserted at left Kocher’s point; and (F) 4 months after discharge, with normal-sized ventricles and VP shunt.
The patient’s mental status and laboratory findings gradually improved. On the 14th HD at 3:25 PM, the EVD was removed, as she responded to all verbal questions and directions (intact place, time, and person orientation, and her motor grade was 4), and she was transferred from the intensive care unit to a general ward. Two hours after EVD was removed, the patient exhibited a sudden deterioration of mental status (deep drowsiness) and presented with an enlarged left ventricle, which was seen on brain CT and received a second EVD insertion. CSF analysis results were as follows: WBC count of 12/μL (PMN, 90%), red blood cell count of 3,500/μL, glucose of 61 mg/dL, and protein level of 29.28 mg/dL. The fluid was pinkish. Later, the neurosurgery team inserted a ventriculoperitoneal (VP) shunt. On HD 28, her GCS score was 15; her motor assessment results were all grade 4; her Mini-Mental State Examination (MMSE) score was 11; her functional ambulation categories (FAC) score was 2. She was transferred to a rehabilitation hospital on HD 91. About 5 months later, the patient’s status improved to a GCS score of 15, motor grades 4, a FAC score of 3.5, and an MMSE score of 21.
Overall, the patient’s antibiotic regimen consisted of ceftriaxone (2 g every 12 hours) and vancomycin (1 g every 12 hours) for 6 days, followed by switching to ampicillin/sulbactam (3 every 6 hours) and ceftriaxone (2 g every 12 hours) for 21 days. Thus, her antibiotic treatment lasted for a total of 26 days.
Discussion
S. paucimobilis can be isolated from seawater, river water, invertebrates residing in water, and water distribution systems, including hospital environments [2]. This organism is often responsible for catheter-associated infections and hospital outbreaks [3,4]. S. paucimobilis infection usually occurs in severely ill patients, including immunocompromised patients, due to its low virulence. Most case reports of S. paucimobilis infection presented with primary bacteremia and were often associated with catheter-associated infections [3,4,8]. Only a few cases of S. paucimobilis central nervous system infection have been reported (Table 1) [4,9-15]. When this pathogen infects the central nervous system and the adjacent tissue, the prognosis varies from baseline function recovery to severe disability and even death [9-11]. The treatment duration for meningitis caused by gram-negative bacteria has not been clearly defined [16].

Case reports of Sphingomonas paucimobilis meningitis
Table 1 contains nine case reports of S. paucimobilis meningitis, including this case. Bacterial meningitis is challenging to diagnose due to its various clinical signs and symptoms [17]. Among these reports, some had normal radiological findings with atypical clinical presentations of meningitis during the first clinical visit, like this case [13,15]. Four out of nine S. paucimobilis meningitis cases were complicated with hydrocephalus [4,10,13].
L. monocytogenes, a foodborne pathogen, is relatively common. More than 70% of listeriosis cases occur in patients with recognized underlying diseases, such as liver disease, cancer, and diabetes [18]. In the current case, the patient had no gastrointestinal symptoms. However, it must be noted that she had breast cancer, for which she had received the last adjuvant chemotherapy 13 months before. Her history of breast cancer and age of 66 years had thus increased her risk of listeriosis [18]. Furthermore, there are several cases of listeriosis that are linked to traditional procedures such as acupuncture [19]. Mixed infections in adult bacterial meningitis were reviewed by Chang et al. [20]. The authors analyzed 12 cases of CSF polymicrobial culture results. They concluded that mixed-infection adult bacterial meningitis was mainly of a nosocomial nature and associated with underlying conditions such as VP shunt.
Two different pathogens were obtained in the CSF and blood from the initial evaluation in the presented patient. Given her past medical history, a coinfection with S. paucimobilis meningitis and L. monocytogenes bacteremia without gastrointestinal signs and symptoms suggested a possible procedure-related infection from the acupuncture and cupping after moxibustion.
Xu et al. [19] reviewed 308 cases of acupuncture, moxibustion, and cupping that were associated with adverse events. One of the most common adverse events in these cases was infection. Traditional procedures, including acupuncture, are often performed by unlicensed people without medical training. There are many open classes and YouTube videos teaching and promoting traditional procedures to the public that do not discuss the concepts of infectious diseases or regulations issued by proper authorities. Public bath places equipped with cupping and moxibustion are ubiquitous. Furthermore, in reviewing this case and other case reports of procedure-related infection, licensed medical practitioners are also responsible for procedure-related infections. The risk of infectious diseases in these settings should be emphasized through proper supervision and education from qualified authorities.
For patients like this, close observation is recommended to initiate surgical treatment without delay. Constant neurological observation, prompt surgical responses, and a suitable antibiotic regimen are essential for treating S. paucimobilis meningitis complicated with hydrocephalus.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization, Methodology, Investigation, Visualization, Resources, Supervision: SWB; Data curation, Validation: SWB, JHL; Writing-original draft: SWB; Writing-review & editing: SWB, JHL.