A comparative study of the psychological impacts of tasks related and unrelated to COVID-19 on nurses: a cross-sectional study
Article information

Abstract
Background
This study assessed the psychological impact of the outbreak of coronavirus disease 2019 (COVID–19) on university hospital nurses. It provides an assessment of mental health issues, including depression, anxiety, distress, and burnout of nurses dealing directly and indirectly with COVID–19.
Methods
In a web-based, cross-sectional study, 111 nurses from Daegu Catholic University Hospital in Korea were enrolled from August 4 to August 9, 2020. Patient Health Questionnaire–9, Generalized Anxiety Disorder–7, Impact of Event Scale–Revised, and Maslach Burnout Inventory were used to assess the psychological symptoms of depression, anxiety, psychological distress, and burnout among the study participants.
Results
Of 111 nurses, 35 (31.5%), nine (8.1%), 26 (23.4%), and 49 (44.1%) experienced depression, anxiety, distress, and burnout, respectively. Nurses who performed COVID–19–related tasks were more likely to have moderate depression (related vs. unrelated, 52.0% vs. 25.6%; p=0.037). There were no differences in anxiety, distress, and burnout between nurses with and without COVID–19–related tasks. More than 50% of the participants showed receptive and positive attitudes toward caring for COVID–19 patients.
Conclusion
Nurses who performed COVID–19–related tasks had a higher risk of depression. There were no significant differences in anxiety, distress, and burnout between the two groups. Since nurses who perform COVID–19–related tasks are more prone to psychological distress, continued psychiatric interventions are required for infectious disease outbreaks with a high mortality rate for healthcare workers who are emotionally vulnerable.
Introduction
In December 2019, a coronavirus disease 2019 (COVID-19) outbreak occurred in Wuhan (Hubei, China) [1]. In early 2020, COVID-19 began to spread rapidly on a global scale. On March 11, 2020, the World Health Organization (WHO) officially declared COVID-19 a pandemic [2]. This rapid and unprecedented pandemic has led to significant mental health problems such as depression and anxiety among healthcare workers (HCWs) and the general population [3,4].
The WHO identified HCWs as a group particularly at risk of developing a wide range of physical and mental problems as a result of working directly or indirectly with COVID-19 patients [5]. HCWs are at the forefront of the fight against infectious diseases and in providing patient care. HCWs are exposed to severe stress, high emotional load, long working hours, the risk of being infected or infecting their families, inadequate support in the work environment, and the lack of effective supportive treatments, all of which affect their mental health [6,7]. HCWs may experience a variety of symptoms, including anxiety, stress, fear, and insomnia [8]. Representing almost half of the global healthcare workforce, nurses are at the forefront of providing care and services across the health spectrum [9]. Thus, their mental health is most likely to be affected. For example, a study revealed that during the peak of the 2003 severe acute respiratory syndrome (SARS) outbreak in Taiwan, nurses treating patients suffered from extreme stress, among other psychological problems [10]. Burnout was reported to be especially high among nurses who worked long hours with the Middle East respiratory syndrome (MERS) patients [11]. A meta-analysis demonstrated that young HCWs who were nurses and women during the SARS/MERS/COVID-19 epidemics/pandemics were particularly vulnerable to SARS/MERS/COVID-19–related psychological distress, including anxiety, depression, and exhaustion [4].
South Korea has been in a state of emergency since February 23, 2020 owing to the COVID-19 crisis. In the Daegu and Gyeongbuk province, a region located in South Korea, the number of people infected with COVID-19 has increased dramatically since the 31st case was confirmed. Approximately 5,300 additional cases were confirmed within 15 days, representing approximately 70% of the total number of confirmed cases. Daegu became the epicenter of the outbreak in South Korea [12]. Innumerable medical workers and resources have been devoted to the efforts to treat COVID-19. To control the spread of COVID-19, the authorities of Daegu carried out various administrative regulations. All citizens in Daegu were asked to self-quarantine and maintain social distancing. South Korea began implementing quarantine measures along with social distancing, especially considering the number of confirmed cases in Daegu since March 22, 2020. As the sporadic cases persisted, the Ministry of Health and Welfare categorized social distancing rules into three stages, with Stage 1 being the least intense and Stage 3 being the most stringent. Stage 3 had to be implemented on June 28, 2020, and schools and companies were urged to close. Since the explosive outbreak, Daegu has maintained a low level of social distancing in daily life.
Due to the ongoing COVID-19 pandemic, HCWs are constantly exposed to the risk of infection, and they need to maintain strict social distancing for several weeks or months. There are numerous studies on the psychological impact of the COVID-19 outbreak on frontline HCWs, particularly nurses. However, few studies have compared the impact of such outbreaks on those who perform tasks directly related to the outbreak versus those who do not. This has left gaps in the existing literature in terms of understanding the different mental health outcomes of different groups of people during such crises. The present study provides an assessment of the mental health burden of nurses working directly and indirectly with COVID-19 patients.
Materials and methods
1. Study design and participants
The study was conducted with medical nurses working at Daegu Catholic University Hospital in Korea during the COVID-19 outbreak. Since the outbreak of COVID-19, the hospital has been in charge of the diagnosis and treatment of COVID-19 (March 1 to May 6, 2020). The survey was conducted from August 4 to August 9, 2020, and data were collected through an online questionnaire distributed to HCWs via a mobile text message. Of the 1,387 HCWs, 500 were selected using a random extraction method, of which 133 responded to the questionnaire. Only one response was permitted per person. Questionnaires with missing information were excluded from the study. Accordingly, 111 participants were enrolled in the study.
2. Measurements
The questionnaire was designed to identify factors that could affect the mental health of nurses. Demographic factors included age, sex, and medical history. COVID-19–related variables included quarantine experience, confirmed COVID-19 cases among family members, and exposure to COVID-19–related tasks. COVID-19–related tasks included working in the isolation ward or screening center and working directly with patients who were positive for COVID-19 or those having a high chance of being infected. Tasks not related to COVID-19 included working in a general ward (non-COVID-19), entrance visitor screening, and working in outpatient departments. These non-COVID-19–related tasks pertain to other consequences of the pandemic and do not involve coming face-to-face with infected patients.
1) Perception of COVID-19 threat
Participants were asked about their perceived threat of COVID-19. The items were adapted from those used in a previous study assessing the psychological impact of SARS on hospital employees [10], including perceived job risk, perceived stigma, perceived job stress, fear of infection, little control, worry about transmission, concern for others, and thought of the possibility of death. The survey consisted of 10 questions rated on a 5-point Likert-type scale ranging from 1 to 5 (1, strongly disagree; 5, strongly agree).
2) Measurement of depression and anxiety symptoms
Patient Health Questionnaire-9 (PHQ-9) is a 9-item self-administered instrument, used to measure depression symptoms [13,14]. Items are rated on a 4-point Likert-type scale ranging from 0 (not at all) to 3 (nearly every day). The total scores range from 0 to 27 (cutoff value ≥10). Generalized Anxiety Disorder-7 (GAD-7) is a tool for assessing the presence of anxiety [15-17]. Items are rated on a 4-point Likert-type scale ranging from 0 (not at all) to 3 (nearly every day). The total scores range from 0 to 21 (cutoff value ≥10). Cronbach’s alpha in the current study was 0.882 and 0.859 for PHQ-9 and GAD-7, respectively.
3) Impact of Event Scale-Revised
The Korean version of Impact of Event Scale-Revised (IES-R) has been used to assess psychological distress among the general population, workers, and psychiatric patients [18]. The IES-R is a 22-item, 6-point scale (0, not at all; 1, a little bit; 2, moderate; 3, quite a bit; and 4, extreme), with a Cronbach’s alpha of 0.967. The total score ranges from 0 to 88. A total score of ≥25 in the Korean version of the IES-R is indicative of posttraumatic stress disorder (PTSD), whereas a score of ≥18 indicates the presence of PTSD-like symptoms [19].
4) Maslach Burnout Inventory-General Survey
Burnout measurement was performed using the Korean version of the Maslach Burnout Inventory-General Survey (MBI-GS) developed by Maslach and Jackson [20]. The validity of the Korean version of the MBI-GS was verified by Shin [21]. Overall burnout was defined as a high score in either the emotional exhaustion or depersonalization subscale (cutoff scores: >13 for emotional exhaustion, >8 for depersonalization, and <18 for personal accomplishment) [22]. Cronbach’s alpha for the current study was 0.784.
3. Statistical analysis
Pearson chi-square test or Fisher exact test was used to determine whether there was a significant difference in basic characteristics, perception of threat, and severity ratings of PHQ-9, GAD-7, IES-R, and MBI-GS between the groups depending on the assignment of COVID-19–related tasks. Statistical analysis was performed using PASW Statistics ver. 18.0 for Windows (IBM Corp., Armonk, NY, USA), and the level of significance was set at 0.05.
Results
1. Demographic characteristics
Of the 500 surveys transmitted, 111 responses (22.2%) were received. The basic characteristics of the respondents according to their participation in COVID-19 treatments are shown in Table 1. Twenty-five respondents (22.5%) performed COVID-19–related tasks. Most respondents in both groups were women in their 20s. Only 28.8% of the participants had educational training for infectious diseases. The group with participants who performed COVID-19–related tasks had more quarantine experience during the COVID-19 outbreak (related vs. unrelated, 20% vs. 5.8%; p=0.044). Most respondents did not have family members who were infected nor did they have comorbidities.
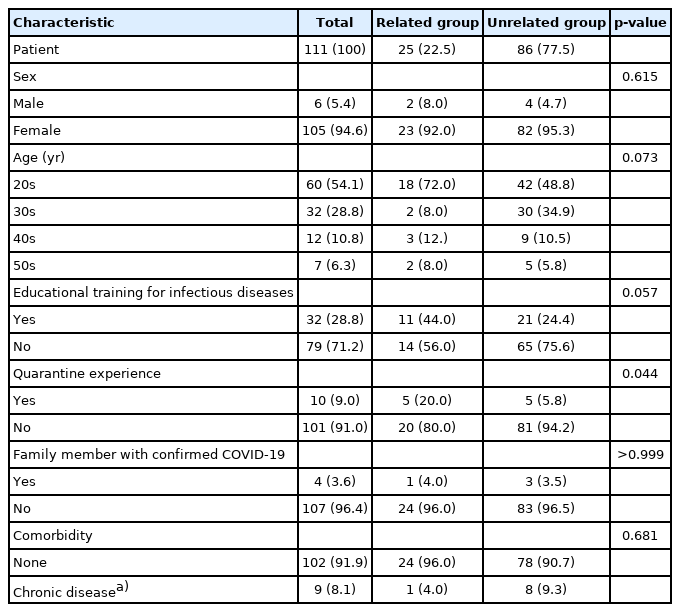
Basic characteristics of respondents according to participation in COVID–19 treatment
2. Perception of COVID-19 threat
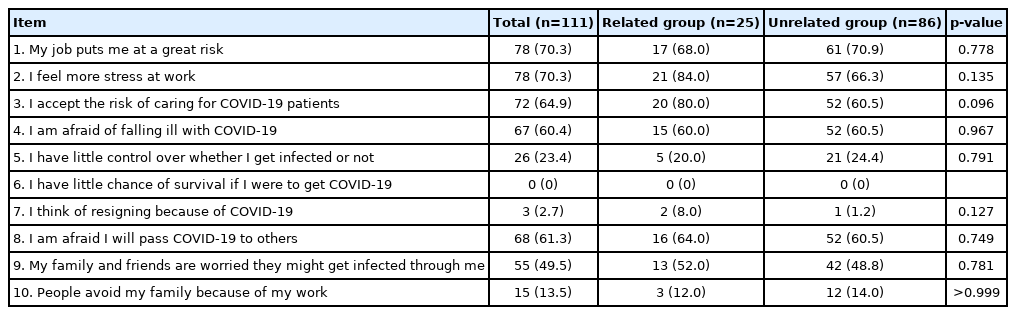
Regarding perceived threat, most respondents felt that their jobs were risky. There was no significant difference between the two groups. Over half of the respondents reported that “My job puts me at a great risk,” “I feel more stress at work,” “I accept the risk of caring for COVID-19 patients,” “I am afraid of falling ill with COVID-19,” or “I am afraid I will pass COVID-19 to others.” The items “I accept the risk of caring for COVID-19 patients,” “I feel more stress at work,” and “I am afraid I will pass COVID-19 to others” showed high proportions in all groups. However, the items “People avoid my family because of my work,” “I have little control over whether I get infected or not,” “I think of resigning because of COVID-19,” and “I have little chance of survival if I were to get COVID-19” showed low proportions in all groups (Table 2).
3. Comparison of depression, anxiety, distress, and burnout among nurses
Table 3 shows the distribution of scores within the PHQ-9, GAD-7, IES-R, and MBI-GS severity cutoffs. The prevalence of mild depression in the COVID-19–related task group was significantly lower than that in the unrelated task group (16.0% vs. 32.6%, p=0.037). However, the prevalence of moderate to severe depression was significantly higher in the related task group (52.0% vs. 25.6%, p=0.037). All respondents had a GAD-7 score of ≥5. Based on a cutoff value of 10, the prevalence of moderate to severe anxiety was 12.0% and 7% in each group, respectively. However, there were no statistically significant differences between the two groups. Twenty-six respondents (23.4%) screened positive for PTSD, 13 (11.7%) for PTSD-like symptoms, 41 (36.9%) for emotional exhaustion, 33 (29.7%) for depersonalization, 40 (36.0%) for low personal accomplishment, and 49 (44.1%) for burnout. There was no significant difference between the two groups in terms of distress and burnout.
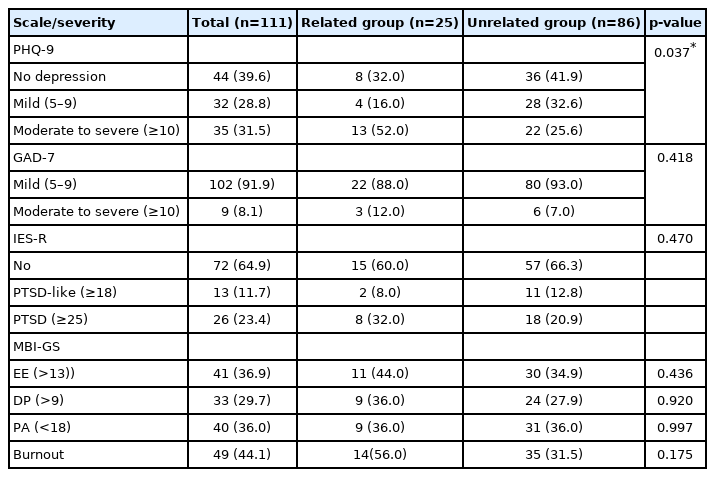
Distribution of nurses across the PHQ–9, GAD–7, IES–R, and MBI–GS severity ratings by group
Discussion
The main outcome of this study indicates that after the COVID-19 outbreak, those who performed COVID-19–related tasks were more likely to have moderate depression. There were no significant differences between the GAD-7, IES-R, and MBI distributions.
In the existing meta-analysis on the psychological impact of COVID-19 on HCWs from 13 studies, the prevalence of depression was 22.8% [23]. The prevalence of depression and anxiety in the current study was 31.5% and 9%, respectively, and nurses involved in COVID-19–related tasks showed a higher prevalence of depression than those who were not involved. Most respondents had mild anxiety (91.9%). This outcome was similar to that of earlier studies, which found that HCW jobs involving close contact with COVID-19 patients can be risk factors for depression and anxiety. Exposure to unspecified patients has also been associated with depression and anxiety [24]. There are some concerns that GAD-7 may not be sensitive to measuring reactive anxiety after stress. However, GAD-7 has the advantage of effectively discriminating anxiety disorders in a short period of time and has been widely used in epidemiologic studies [25].
The prevalence of PTSD-like symptoms, PTSD, and burnout among respondents was 11.7%, 23.4%, and 44.1%, respectively. There were no statistically significant differences between the two groups. Previous studies on the impact of COVID-19 on the mental health of HCWs have indicated that frontline HCWs who provide direct care to COVID-19 patients are at a higher risk of distress and burnout [26,27]. Women, nurses, and young people have greater psychological distress than men and physicians, as the formers are thought to be more vulnerable to stress [24,28]. Considering reasons the results differ from those of previous studies, the participants’ receptive attitude toward the disease and educational training on infectious diseases may have acted as protective factors. In the case of the COVID-19–related task group, a significant proportion of the responses agreed with the item, “I accept the risk of caring for COVID-19 patients” and disagreed with the items, “I have little control over whether I get infected or not” and “I think of resigning because of COVID-19,” indicating that they are receptive and positive toward taking care of COVID-19 patients. Since the COVID-19–related task group was mainly engaged with high-risk infectious disease and received infectious disease education, as opposed to the other group, the effect on mental health may have been offset.
Furthermore, considering that this study was conducted during Stage 1 of social distancing norms, psychological adaptation may have occurred over time. In the Daegu-Gyeongbuk region, minor local infections have continued since the explosive spread in February 2020 [29]. Regarding SARS, a study on 1,257 HCWs reported differences in mental health across the two phases of the outbreak. In the initial phase, when the disease spread rapidly, 81% of the participants experienced anxiety. During the repair phase, when the infection was brought under control, 77% experienced anxiety. The decreasing anxiety was thought to be the result of the virus being under control and the increasing recognition that the disease was preventable [30]. A Chinese study on frontline nurses supplying care to patients with COVID-19 also recorded psychological changes over time; psychological adaptation was observed during the later stage. This might be mainly due to the familiarity of the nurses with the work environment and processes, the mutual support of team members, monetary incentives, social support, and recognition from the government and public. They felt that what they were doing was important and valuable to the health of the people and the nation. Their energy was renewed by rediscovering the original purpose of their dedication to care, reevaluating the nursing profession, taking pride in their contributions, and having an upgraded sense of personal accomplishment [31].
This study has some limitations. First, the sample size was small and may not be representative of the psychological states of all nurses. In addition, differences in mental status according to the tenure of the nurse or the type of work were not included in the study. Further investigations with a larger sample size and detailed classification are needed. Second, the study design did not include an analysis of the causes of psychological strains, such as work-related stress. Further studies on the various factors that may affect the psychological status of nurses are needed. Third, this study was cross-sectional, so it was unable to distinguish pre-existing mental health symptoms from new symptoms. Considering the long duration of COVID-19, the psychological status of nurses can change over time. It would be ideal to reinvestigate the mental health of nurses after a period of time, including long periods of depression, anxiety, stress, and burnout. It is important to highlight the importance of designing interventions that target female nurses who work directly with infectious diseases, as they may experience higher psychological burdens.
The COVID-19 pandemic had negative psychological implications for nurses who performed COVID-19–related tasks. They showed a higher risk of depression, but anxiety, distress, and burnout were not significantly different between the two groups. Continued psychiatric interventions of emotionally vulnerable groups among HCWs are required for infectious disease outbreaks.
Notes
Ethical statements
The Institutional Review Board of Daegu Catholic University Hospital (IRB No: CR-20-109) reviewed and approved this study. Informed consent was obtained from all respondents.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Author contributions
Conceptualization, Formal analysis: HJK, GHL; Data curation, Methodology, Visualization, Investigation, Resources, Software: HJK; Funding acquisition, Supervision, Validation: GHL; Writing-original draft: HJK; Writing-review & editing: HJK.