Factors associated with musculoskeletal pain in professional dancers, including lapse period of group practice due to the COVID-19 outbreak: repeated-measures analysis
Article information

Abstract
Background
This study investigated the prevalence and associated factors of musculoskeletal pain among professional dancers who experienced a lapse in group practice due to coronavirus disease 2019.
Methods
General characteristics, practice time, region of musculoskeletal pain due to injury using the visual numeric scale (VNS), and causative motion were surveyed among professional dancers. Pain of VNS 0 to 3 was categorized as “no or minor,” 4 to 6 was categorized as “moderate,” and 7 to 10 was categorized as “severe.” The causal motions of musculoskeletal pain were analyzed according to body region. Factors other than motion associated with pain were also analyzed.
Results
In total, 368 participants were included. In the univariate analysis, age and practice time were positively associated with “moderate” pain. Practice time, dance experience, and postural accuracy were positively associated with “severe” pain, as was performing Korean traditional dance. In the multivariable analysis, practice time, group practice, and age were positively associated with pain of VNS 4 to 10, and practice time, group practice, and Korean traditional dance were positively associated with pain of VNS 7 to 10.
Conclusion
Among the factors related to dancer training, practice time, group practice, and dance type affect the occurrence of pain.
Introduction
Dancers are both athletes and artists [1] who pursue aesthetic expression through body movements and postures, which often cause their muscles and joints to function above the average physical capability of the general population [2]. Athletes practice to improve their physical condition and achieve a high level of performance in competition, while dancers must continuously practice their movements and postures harmoniously and beautifully in the pursuit of artistic perfection. Furthermore, general athletes have a season in which they prepare for competitions to produce the best performance, and a season in which they physically recover after the competition is over. Thus, they experience a cycle of seasons requiring different physical effort. However, dancers prepare year-round for various performances without an off-season and require continuous and cumulative practice to improve performance quality [3]. Thus, dancers are at a higher risk of sustaining musculoskeletal injuries than general athletes.
Numerous investigations have elucidated an elevated incidence of musculoskeletal disorders (MSDs) among dancers. Despite the variability in outcomes attributed to the divergent methodologies and geographical locations of these studies, the consensus indicates a pronounced prevalence of MSDs within this cohort throughout their careers. A previous study indicated a lifetime prevalence of 54.8% for MSDs in professional ballet dancers, with modern dancers exhibiting a slightly lower rate of 46.3% [4]. Notably, a specific examination of professional ballet practitioners in Sweden revealed an exceedingly high lifetime MSD prevalence rate of 95% [5,6]. Furthermore, a comprehensive systematic review of the extant literature revealed that approximately 50% of professional dancers experience low back pain during their lifetimes [7]. The discourse surrounding MSDs in dancers often categorizes these ailments as occupational diseases [3,8], highlighting the significantly higher prevalence of MSDs in this profession than in other occupational sectors. For instance, the incidence of nonfatal occupational injuries and illnesses necessitating absence from work among dancers is reported to be 343.2 cases per 10,000 full-time equivalent workers, markedly surpassing the rates observed in the general occupational population (120.7 cases), among carpenters (202.7 cases), and among construction laborers (207.1 cases) [9].
Several studies have indicated risk factors related to the prevalence of these MSDs, such as posture, flexibility [10], body type, sociopsychological factors [11], dance exposure, age, joint range of movement, and anthropometrics [12], although these have not yet been clearly established. In this study, the prevalence of musculoskeletal pain due to injury among professional dancers performing modern dance, ballet, and Korean traditional dance in the Republic of Korea was surveyed using a self-administered questionnaire, and the influencing factors were analyzed. In early 2020, coronavirus disease 2019 (COVID-19) severely curtailed performing activities, leaving most dancers in a lapse period without performances and group practice. During this period, dancers took a break from rehearsals and either focused on individual practice or rested. As the spread of COVID-19 decelerated, dancers returned to their regular professional practice. This study investigated the prevalence of musculoskeletal injuries and pain among dancers, considering both the period of professional practice and the lapse period of group practice due to COVID-19.
Methods
Ethical statements: The authors obtained approval from the Institutional Review Board (IRB) of Yeungnam University Hospital (IRB No: YUMC 2021-04-005-001). All the participants provided written informed consent.
1. Study participants
This investigation was undertaken among professional dancers actively engaged in routine dance practices and affiliated with nine distinguished dance companies in the Republic of Korea. The temporal scope of this study spanned from July to August 2021. By employing a retrospective recall methodology, this study targeted two specific timeframes. The initial period was March to April 2020, during which collective practice sessions ceased in response to the COVID-19 pandemic. The subsequent interval extended from February to March 2021, a phase characterized by the resumption of regular group practices. Notably, the first COVID-19 case in Korea was documented in February 2020, followed by the implementation of restrictions on public gatherings and the promulgation of "social distancing" directives in March 2020 [13]. During the first survey period of this study (March to April 2020), no group practices, including remote meetings using mobile and personal computer platforms, were conducted. In contrast, March to April 2021 was the period when group practices were normally conducted with dancers required to wear masks, given the Korean government’s requirement for wearing masks indoors.
This study surveyed professional dancers specializing in ballet, modern dance, and Korean traditional dance. Regarding college students, this study excluded individuals majoring in dance without professional engagement. The inclusion criteria were strictly limited to college students who were members of collegiate dance ensembles and demonstrated a commitment to performing and practicing at a volume and intensity commensurate with that of professional dancers affiliated with a dance company.
A researcher visited a company that agreed to participate in the research, confirmed that each member had agreed to participate, explained the purpose of the research to the consenting participants, and obtained consent to proceed. Printed structured questionnaires were distributed and self-completed by consenting participants. Submitted questionnaires were excluded from the analysis if there were missing values for the variables of interest, except for flexibility and posture accuracy; in some questionnaires, only flexibility and posture accuracy items were missing. When all other items were completed, statistical imputation was performed, and the survey was included in the analysis.
2. Survey
The self-administered questionnaire involved general demographics and dance-specific attributes, including sex, age, years of dance experience, height, weight, current affiliating institution, style of dance, duration of practice sessions (pertaining to each of the delineated periods), locations of pain experienced, and the visual numeric scale (VNS) pain assessment. Data were collected from July to August 2021 using recall methodology to investigate the two predetermined periods of interest.
Regarding practice time, the lapse of group practice and performance between the first 2 months, February and March of 2020, of the COVID-19 outbreak (“lapse of group practice” period) and the period after return to regular practice for 2 months in March and April 2021 (“after return” period) was investigated. Each participant was assessed for musculoskeletal pain due to injury during the “lapse of group practice” and “after return” periods. The survey was conducted using a structured questionnaire. Regarding the regions of pain due to injury, participants could choose from 13 regions in the questionnaire, including (1) neck, (2) shoulder, (3) elbow, (4) wrist/hand, (5) back/trunk, (6) waist/pelvis, (7) hip joint, (8) thigh, (9) knee, (10) calf, (11) ankle, (12) foot/toe, and (13) other. A 0 to 10 VNS was used to investigate pain intensity. A maximum of three regions were assessed and assigned a pain score. Questions assessing joint flexibility and postural accuracy were based on the Beighton score [14] and dance technique motor control test, respectively, which have been validated for inner-rate reliability and used in a previous study on musculoskeletal pain among dancers. Flexibility was scored on a scale of 0 to 9, and postural accuracy ranged from 0 to 13, according to the previous study [10].
3. Variable categorization and statistical analysis
First, the general characteristics of the participants, including sex, age, dance style, affiliation, number of years of professional dancing, practice time for each period, height, weight, flexibility, and postural accuracy, were assessed. There were three and seven cases that did not respond to questions regarding flexibility and postural accuracy and, since they responded faithfully to other items, statistical imputation was performed using the “predictive mean matching” method.
Referring to the literature, those who described pain as 0 to 3, 4 to 6, and 7 or higher on the VNS were classified as “no or minor,” “moderate,” and “severe” pain, respectively [15]. The prevalence of pain caused by injury was calculated separately. Specifically, the investigation was conducted by subdividing the injuries based on where they occurred on the body. The analysis was performed by classifying body regions by considering the low injury prevalence to each region during the group practice period.
For musculoskeletal symptoms, categorization was performed as follows:
ꞏ Neck and back/trunk were classified as “upper trunk”
ꞏ Shoulder, elbow, and wrist/hand were classified as “upper limb”
ꞏ Waist/pelvis and hip were classified as “lower trunk”
ꞏ Knee, thigh, calf/ankle, and foot/toe were classified as “lower limb”
ꞏ If any of the above items were checked in the survey, it was marked as “any part”
Considering the high rate of lower limb injuries among dancers, this category was divided into two subgroups: knee and calf as “proximal lower limb” and ankle and foot/toe as “distal lower limb.” Cases of pain in one or more regions in each category were counted. Therefore, the total number of subcategories was not necessarily equal to the total number of upper categories. For example, if an individual described pain in the shoulder, knee, and thigh, this would be counted as one in the “any parts” group, one in the “upper limb” group, and one in the “lower limb” group. The prevalence of pain by body region in the “lapse of group practice” and “after return” periods was compared using McNemar test.
To identify musculoskeletal risk factors other than movement, the sex, dance style, age, experience, practice time, flexibility, accuracy, height, and weight of participants in each pain group were classified using the VNS for pain (“no or minor,” “moderate,” and “severe”). These categorizations were compared. The pain group classification was based on the region with the highest VNS among the three regions based on the participants’ responses.
An analysis of variance or the Kruskal-Wallis test (for the “lapse of group practice” period, which had only four participants with severe pain) was used for continuous variables. The chi-square and Fisher exact tests (when the predicted number for each category was five or fewer) were used for categorical variables to compare the characteristics of the groups with “no or minor,” “moderate,” or “severe” pain. The statistics and p-values for each method were calculated.
A multivariable model was used to calculate variables showing potential associations with pain in the univariate analysis. The model was calculated separately by coding the outcome variables binomially with or without “moderate” and “severe” pain. A generalized linear mixed model (GLMM) with logit link function was used to calculate an integrated model, including each practice time and pain for the “lapse of group practice” and “after return” periods. The dependent variable, pain, was based on the classification of moderate or severe pain in the univariate analysis. However, if only moderate pain was set as the dependent variable, severe pain should be grouped into the “no or minor pain” group or analyzed after excluding the severe pain group. The former method may cause bias that underestimates the risk, whereas the latter method has the disadvantage of removing approximately one-third of the samples. Thus, the dependent variable was analyzed by classifying cases where the VNS scored 4 points in one or more sites in model 1 and cases where the VNS scored 7 points or more in one site in model 2.
A random intercept model was used in which each participant was regarded as a random effect. The Akaike information criterion cannot be compared in a GLMM with different fixed effects [16]; therefore, we performed manual purposeful variable selection [17]. The multivariable model was calculated using variables that showed potential significance (p<0.15) in the univariate analysis. Variables with the highest p-values were removed sequentially, leaving those with potential significance. Then, leaving only potentially significant variables, the removed variables were included individually to check whether they were potentially significant in the model [18]. Categorical independent variables composed of more than two categories were included when at least one of the categories had a p-value <0.15. In the case of body weight and weight, the effect of sex was significant; thus, they were excluded when the sex variable was not included.
Statistical analyses were performed using the IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA) 0 and R project 4.2.1 (https://www.r-project.org) were used. The packages used for each statistical analysis were “lme4” [19] for the GLMM package and “mice” [20] for missing value imputation.
Results
1. General characteristics
A total of 405 participants were surveyed, and 368 participants were included in the study; 37 participants who had missing values for the variables of interest were excluded. In seven participants, only flexibility and postural accuracy items were missing, which were relatively difficult to answer, and there were no missing values for any other variables of interest; thus, statistical imputation was performed for these participants. The survey was conducted among five college dance teams and four dance companies.
This study included 79 male (21.5%) and 289 female subjects (78.5%). In terms of dance style, 216 (58.7%) performed modern dance, 74 (20.1%) ballet, and 78 (21.2%) Korean traditional dance. The average practice time was 4.7±6.1 hours per week during the “lapse of group practice” period and 18.5±12.1 hours per week during the “after return” period. During the “lapse of group practice” period, 127 out of the 368 participants did not practice. The characteristics of the participants are presented in Table 1.

General characteristics of participants
2. Prevalence of pain due to injury
Table 2 presents the comparison of pain by body region during each period. Fifty (13.6%) and 187 participants (50.8%) experienced “moderate” pain during the “lapse of group practice” and “after return” periods, respectively (p<0.0001). Pain in the lower trunk and lower limbs was the most common pain experienced during the “lapse of group practice” period, and pain in the upper limbs was the most common pain experienced during the “after return” period.

Prevalence of musculoskeletal pain due to injury by body region
Severe pain was experienced by four participants (1.1%) during the “lapse of group practice” period and 93 participants (25.5%) during the “after return” period (p<0.0001). In the “after return” period, severe pain was reported the most in the lower limbs, followed by the lower trunk, and finally the upper limbs.
3. Factors related to musculoskeletal pain
To identify the factors related to pain, the characteristics of the groups with “moderate” and “severe” pain were compared (Table 3). Practice time (p<0.0001) and age (p<0.01) had a significant relationship to pain during the “lapse of group practice” period. Factors significantly related to pain during the “after return” period included dance style (p<0.01), age (p<0.05), number of years dancing (p<0.05), postural accuracy (p<0.05), and practice time (p<0.0001). “Moderate to severe” pain was experienced by 100% of the dancers whose practice time after returning exceeded 20 hours per week. “Severe” pain during the “lapse of group practice” period also had a significant positive relationship with practice time. In the case of “severe” pain during the “after return” period, there was a significant relationship between dance style and practice time. In both periods, 100% of the dancers experienced “severe pain” for more than 40 hours per week. The association pattern between practice time and pain during the “after return” period is presented in Fig. 1.

Univariate analysis between pain prevalence and factors other than movements
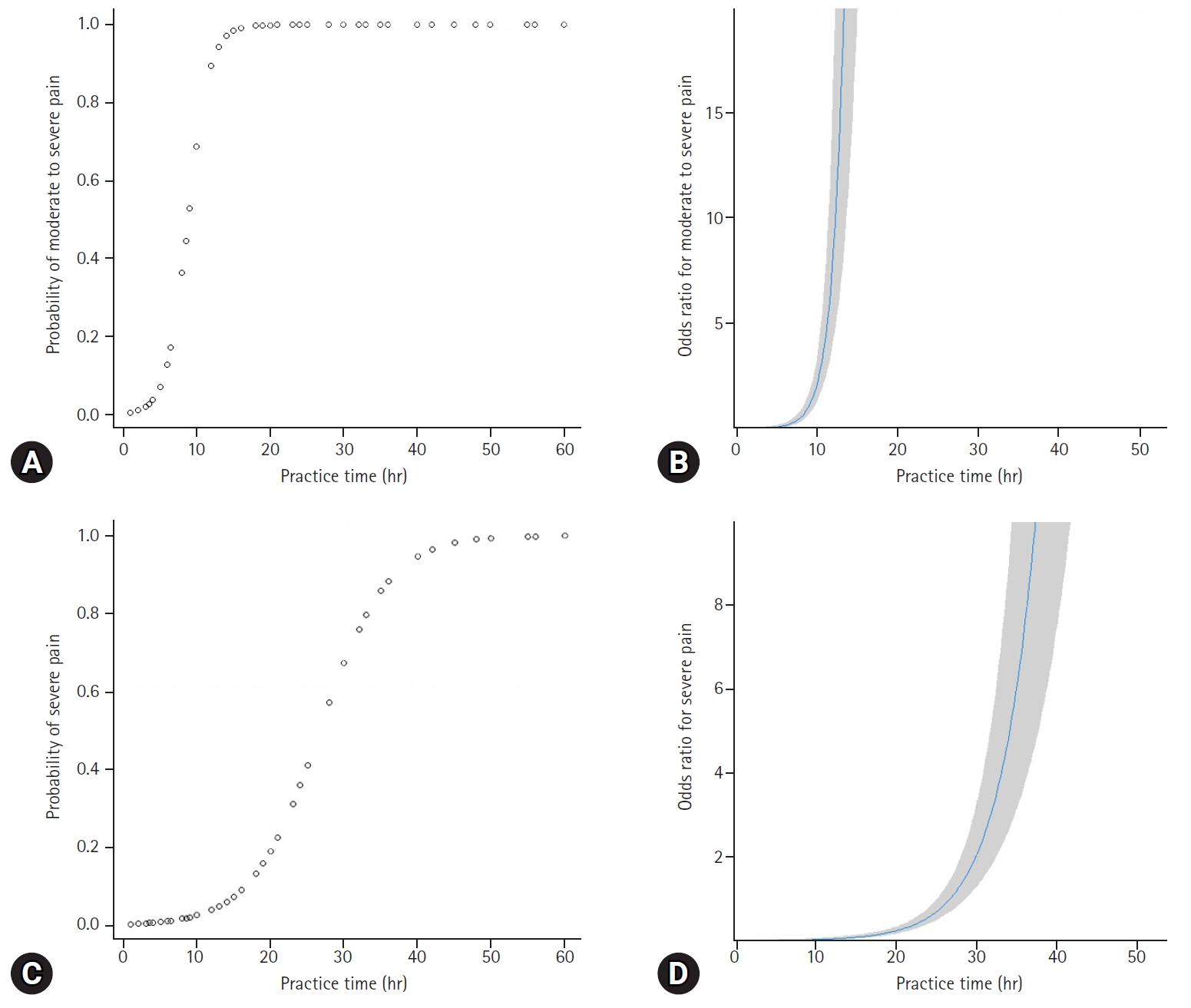
The pattern of association between practice time (hours per week) and musculoskeletal pain in the logistic regression model. (A) Expected probability of “moderate to severe” pain by practice time. (B) Odds ratio for “moderate to severe” pain by practice time. (C) Expected probability of “severe” pain by practice time. (D) Odds ratio for “severe” pain by practice time. “Moderate to severe” pain refers to pain of 4–10 on visual numeric scale (VNS). “Severe” pain refers to pain of 7–10 on VNS.
4. Multivariable analysis
The initial model is shown in Supplementary Table 1. The final model is presented in Table 4. In the final model, practice time had a statistically significant positive relationship with “moderate to severe” pain (odds ratio [OR], 1.84 per hour per week; 95% confidence interval [CI], 1.64–2.06). The incidence of pain was significantly lower in dancers in their 20s than in those in their teens (OR, 0.43; 95% CI, 0.21–0.90). There was a greater prevalence of pain during the “after return” period than during the “lapse of group practice” period (OR, 2.24; 95% CI, 1.13–4.44). Practice time had a significant positive association with “severe pain” (OR, 1.28; 95% CI, 1.21–1.34), and there was a significantly greater prevalence of pain in the “after return” period than in the “lapse of group practice” period (OR, 9.46; 95% CI, 1.51–59.19). There was also a significantly greater prevalence of pain among dancers practicing Korean traditional dance than among those practicing modern dance (OR, 2.83; 95% CI, 1.16–6.94).

Final multivariable model of pain prevalence and potentially associated factors by generalized linear mixed model
Discussion
This study investigated factors affecting the prevalence of pain due to injury among professional dancers who had a lapse period due to COVID-19 and later returned to regular practice. A mixed model approach was used in this study. One advantage of using a mixed model to analyze repeated-measures data is the ability to analyze each participant’s repeated measurements as individual cases, akin to cases in different states. In the context of the COVID-19 pandemic, this study provides an opportunity to analyze the sudden cessation of practice among professional dancers as a unique circumstance. This allowed the use of this group as an internal control to analyze the impact of practice on musculoskeletal pain. During the “lapse of group practice” period, individual practices, or possibly unofficial small group practices, were performed; regular practice was performed after practices resumed. Therefore, it is possible to analyze the effect of the practice type on pain. There was also an opportunity to assess the prevalence of pain according to various practice times due to a sharp decrease in practice time during the “lapse of group practice” period.
A positive correlation was identified between practice time and pain. These results are similar to those of previous studies. Many previous studies have reported that the practice time of dancers is a particularly important risk factor for musculoskeletal symptoms. Kadel et al. [21] reported that dancing for more than 5 hours per day increased the risk of stress fractures in professional ballet dancers. It has been reported that both cumulative training periods and weekly practice time increased injuries among professional dancers in the United Kingdom [22]. However, in previous studies conducted in the Republic of Korea, it was difficult to identify the relationship between practice time and pain because dancers participated in regular professional training. Kwon [23] reported that the practice time and number of performances did not affect musculoskeletal pain. However, in the present study, by analyzing the data, including lapse of group practice and performance time for dancers due to COVID-19, it was possible to examine the relationship between musculoskeletal pain and practice time, including during the period when practice time had decreased to 0 hours per week. Practice time was in the form of a “dose-response curve” and appeared as a threshold model, in which most of the pain experienced by dancers occurred when a certain amount of practice time was exceeded. The risk of “moderate or severe” pain, unless the practice time was less than 10 hours per week, increased rapidly with practice time, and the threshold at which pain always occurred was approximately 20 hours per week. For “severe” pain, when practice time was less than 20 hours per week, there was a relatively gentle increase followed by a steep increase; the threshold at which “severe” pain always occurred was approximately 40 hours per week of practice time.
Unlike other athletes who train mainly with drills rather than full games during practice and train their bodies to achieve maximum performance during practice, the training or practice of dancers differs little from actual performance. In the case of dancers, the possibility of injury during practice is considered to be higher than that of athletes because dancers practice at the level of performance [3]. In athletes, although there are exceptions depending on the sport, the incidence of injuries during games is generally reported to be 2 to 4 times higher than that during practice [24-26]. In dancers, injuries occurring during performances are more likely than those occurring during rehearsals. However, it has been reported that injuries during dancers’ performances contribute to approximately 50% of total injuries, and the contribution of rehearsal or practice injuries is regarded to be relatively higher among dancers than among athletes [3,27]. During the “after return” period, in which regular and professional practices were performed, pain seemed to increase independently of practice time compared to that experienced by dancers during the “lapse of group practice” period, in which individual or small group practices were performed. The significant difference in the prevalence of musculoskeletal pain between these practice patterns may provide an important basis for classifying the pain caused by regular practice as a work-related symptom. Another study produced results that showed that social distancing due to COVID-19 led to musculoskeletal pain due to psychological factors and lifestyle changes [28]; however, in the present study, the prevalence of pain in all body regions was significantly lower during the COVID-19 period when group practice was not held.
When performing during group practices, “moderate” and “severe” pain appeared most frequently in the lower limbs, followed by the lower trunk. Shah et al. [29] reported that injuries occurred most frequently in the ankle, followed by the waist and knee in professional modern dancers. Ramel et al. [30] reported that 69% to 82% of professional ballet dancers sustained lower back injuries and 73% to 82% reported musculoskeletal pain in the foot. Kwon [23] reported that back, leg, and ankle pain were most severe in college students majoring in dance. Wanke et al. [31] reported that the ankle is the most frequently injured region, and that jumping is the movement that causes the most injuries among ballet dancers. Motta-Valencia [32] reported that the upper extremities were mainly injured during lifting maneuvers, and the lower extremities were mainly injured during jumps or landings. Although there were some differences due to different participant characteristics and outcomes in each study, the findings that severe injuries occur frequently in the lower extremities and lower back are consistent with the results of our study.
A higher risk of “severe” pain was identified among Korean traditional dancers. Korean traditional dance involves movements that are completely different from those of modern dance and ballet. However, few studies have reported the effects of these movements on MSDs. One study examined exercise intensity in Korean dancers. In a study of 20 female college students with more than 5 years of dance experience, the maximum heart rate for each movement was 135.40±4.44 beats per minute (bpm) to 183.35±3.11 bpm, indicating a wide range but that the exercise intensity was high [33]. Although a direct comparison is difficult owing to the different research methods employed, the superior-inferior ground reaction force exceeded 500 N to 1,000 N in some Korean dance movements [34]. This is quite high compared to that reported for ballet dancers (150 N) [35]. The pattern and linkage between basic movements vary depending on the type of dance practiced; thus, the relationship between injury and dance movements in Korean traditional dance should be studied further.
This study had several limitations. From the point of view of the research design, the study was conducted using a survey that was completed via recall. Recall bias may have occurred because both past and current pain were investigated using a single questionnaire. Regarding the outcome, objectivity and specificity may have been lowered by reporting musculoskeletal pain due to injury through self-written questionnaires without referring to medical records. One limitation of our survey questionnaire method is that we did not separate students from professional dancers, although we included only students who belonged to a public or private dance team and had practice and performance equivalent to that of professional dancers. In addition, in the case of group practice, the classification of practice aspects such as rehearsal and technique lessons was not separated in the questionnaire. In the case of a lapse in the group practice period, there may have been an unofficial small group that continued practicing, but this was not reflected in the survey questionnaire. Furthermore, by examining only up to three pain areas, some cases of pain may have been omitted. Because a self-administered method was used, some questionnaire responses may have been omitted either intentionally or inadvertently. Additionally, participants may have experienced difficulties interpreting items such as flexibility and postural accuracy in the questionnaire, although detailed pictures and evaluation methods were provided. The definition of pain was described as “repeatedly injured area and average pain intensity” in the questionnaire. The definition of “injury” was not clarified, and therefore, delayed onset muscle soreness due to simple overuse may have been included. Regarding the statistical methods, owing to the rare research design using the lapsed period caused by COVID-19, a sophisticated sample size or power calculation through similar studies in the past could not have been made in advance.
This study found that practice time and pattern were related to musculoskeletal pain due to injury. We suggest implementing a plan to prevent musculoskeletal symptoms in dancers. First, as increased practice time is an important cause of musculoskeletal symptoms, dance practice should be managed. After showing a linear “dose-response pattern” until a certain time, moderate pain was reported by 100% of dancers completing >20 hours per week of practice, and severe pain was reported by 100% of dancers completing >40 hours per week of practice. Thus, monitoring of musculoskeletal symptoms is required in groups with long practice times.
Second, based on these statistics, dance companies must continuously monitor pain and symptoms while promoting training methods to reduce the burden on frequently injured areas. For example, because single-person dynamic movement is often the cause of musculoskeletal symptoms, attention should be paid to damage and movements that are aesthetically excellent and have less impact on the body. Third, as more pain is experienced by dancers participating in regular practice than by those participating in individual practice (regardless of practice time), the increased risk of musculoskeletal injury sustained during regular practice should be recognized. Although the prevalence of musculoskeletal injury and pain among dancers is high, the tendency to recognize MSDs during practice as a stigma is still prevalent among dancers, preventing early diagnosis [36]. Therefore, similar to the screening programs for the early detection of musculoskeletal diseases, such programs could be helpful for dancers. Efforts have already been made to apply programs used by athletes to treat musculoskeletal symptoms and injuries in dancers [37], although they are still often poorly managed [38]. In the Republic of Korea, no program has been proposed to prevent musculoskeletal injuries in professional dancers. Therefore, it is necessary to develop an appropriate program suitable for the domestic environment and increase awareness to support the application of these programs.
This study identified the prevalence and risk factors for musculoskeletal pain in professional dancers. “Moderate” and “severe” pain showed the highest prevalence in the lower limbs. Single-person dynamic movements caused the most injuries in all body regions. Weekly practice time had a significant positive relationship with musculoskeletal pain, and regular professional practice increased the risk of pain. Among the three dance styles, Korean traditional dancers were at the greatest risk of experiencing “severe” pain compared to modern dance. These results may be used for the future development of musculoskeletal injury prevention or monitoring programs for professional dancers.
Supplementary materials
Supplementary Table 1 can be found at https://doi.org/10.12701/jyms.2024.00171.
Initial multivariable model of pain prevalence and potentially associated factors by generalized linear mixed model
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This work was supported by a 2023 Yeungnam University Research Grant (222A480008).
Author contributions
Conceptualization: YC, JS; Data curation: KB, YC; Formal analysis: YC; Funding acquisition: JS; Methodology: KB, JS; Project administration: JS; Writing-original draft: KB, YC; Writing-review & editing: JS.