E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(4); 2023 > Article
-
Review article
Multidisciplinary approach to sarcopenia: a narrative review -
Wook Tae Park
 , Oog-Jin Shon, Gi Beom Kim
, Oog-Jin Shon, Gi Beom Kim -
Journal of Yeungnam Medical Science 2023;40(4):352-363.
DOI: https://doi.org/10.12701/jyms.2023.00724
Published online: September 7, 2023
Department of Orthopedic Surgery, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding author: Gi Beom Kim, MD, PhD Department of Orthopedic Surgery, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3640 • Fax: +82-53-628-4020 • E-mail: donggamgb@hanmail.net
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,510 Views
- 147 Download
Abstract
- Sarcopenia is a condition in which muscle mass and strength are decreased and muscle function is impaired. It is an indicator of frailty and loss of independence in older adults. It is also associated with increased physical disability, which increases the risk of falls. As a multifactorial disease, sarcopenia is caused by a combination of factors including aging, hormonal changes, nutritional deficiencies, and physical inactivity. Understanding the underlying pathophysiology of sarcopenia and identifying its different causes is critical to developing effective prevention and treatment strategies. This review summarizes the pathophysiology, consequences, diagnostic methods, and multidisciplinary approaches to sarcopenia.
- Skeletal muscle is naturally wasted with age, and after the age of 65 years, this loss accelerates and can lead to negative consequences such as physical disability, falls, poor quality of life (QoL), and death [1,2]. Sarcopenia, characterized by the loss of skeletal muscle mass, strength, and function [3], is a common yet underrecognized age-related condition affecting millions of older adults worldwide [4,5]. The prevalence of sarcopenia increases with age, affecting approximately 10% of adults over the age of 65 years and up to 50% of those over 80 years [6,7]. Given the rapidly aging global population, sarcopenia poses significant challenges to individual health and well-being, as well as healthcare systems and economies [8,9].
- As a multifactorial condition, sarcopenia arises from a complex interplay of factors, including aging, hormonal changes, nutritional deficiencies, and physical inactivity [10-12]. Understanding the underlying pathophysiology and identifying the various causes of sarcopenia are crucial for developing effective prevention and treatment strategies. From this perspective, a multidisciplinary approach to sarcopenia may be needed. Therefore, this narrative review aims to provide a comprehensive overview of the current understanding of causes, consequences, and multidisciplinary approaches of sarcopenia, while also highlighting future directions for research and public health initiatives.
Introduction
- The pathophysiology of sarcopenia is multifaceted and not yet fully understood. However, it is known to involve the interplay of various factors that contribute to the decline in muscle mass, strength, and function. This section will delve into the key aspects of sarcopenia pathophysiology, including muscle mass decline, decreased muscle strength, reduced muscle function, and contributing factors.
- 1. Decline of muscle mass
- Aging results in a progressive loss of muscle mass, with studies suggesting a reduction of approximately 3% to 8% per decade after the age of 30 years. This decline accelerates after the age of 60 years [13]. The age-related loss of muscle mass is not fully understood, and much research is still needed. The loss of muscle mass occurs due to a combination of factors, such as a decrease in the size and number of muscle fibers, particularly type II (fast-twitch) fibers, which are responsible for high-intensity, short-duration activities [11].
- 2. Decreased muscle strength
- Muscle strength declines alongside muscle mass, resulting in a reduced capacity to generate force. This decline in strength is more pronounced in type II muscle fibers, leading to significant impairments in physical performance and mobility [14]. The decrease in muscle strength is influenced by both intrinsic (muscle-related) and extrinsic (neural and hormonal) factors [15,16]. Decreased muscle strength refers to a reduction in the ability of muscles to generate force. It can be caused by a number of factors, including aging, a sedentary lifestyle, certain medical conditions, and poor nutrition. Muscle mass and strength naturally decline with age, and a condition in which this change is rapid can be considered an aspect of sarcopenia.
- 3. Impaired muscle function
- Sarcopenia also affects muscle function, which encompasses various aspects of muscle performance, such as power, endurance, and coordination [14]. Age-related changes in muscle architecture, the neuromuscular junction, and motor unit remodeling contribute to the decline in muscle function [17-19]. Moreover, the impaired ability to repair and regenerate muscle tissue after injury or disuse exacerbates the decline in muscle function in older adults [20,21].
- 4. Contributing factors
- Several factors contribute to the pathophysiology of sarcopenia, as follows.
- Age-related changes in muscle fibers, motor units, and the neuromuscular junction predispose older adults to sarcopenia.
- Hormones such as testosterone, estrogen, growth hormone (GH), and insulin-like growth factor-1 (IGF-1) play crucial roles in maintaining muscle mass and function. The decline and dysregulation of these hormones can lead to sarcopenia [22,23]. The effects of testosterone on skeletal muscle can be explained by its anabolic effects, such as the differentiation of mesenchymal pluripotent cells, and its effects on motor neurons, such as the promotion of nerve regeneration [24]. The decline in testosterone levels with age causes a loss of muscle mass and strength. Estrogen is sometimes converted to testosterone, which is anabolic for muscle protein synthesis and can suppress inflammatory cytokines, which are catabolic for skeletal muscle. After menopause, women experience an accelerated loss of muscle mass and strength, which can be attributed to hormonal changes as well as a decrease in physical activity [25]. The role of GH in skeletal muscle function can be explained by its anti-inflammatory and anabolic effects. In particular, the effects of GH on muscle are mainly mediated by IGF-1, which is secreted by the liver and skeletal muscle and has a hypertrophic effect on skeletal muscle. In addition, secreted IGF-1 significantly downregulates proinflammatory cytokines such as tumor necrosis factor alpha and interleukin-1 beta [26]. In acute sarcopenia, such as following an acute illness or surgery, cortisol acts as a mediator of protein catabolism. Hypercortisolemia can promote loss of muscle mass and strength [27]. Acute pain or inflammatory reactions can stimulate the hypothalamic-pituitary-adrenal axis, leading to homeostatic and metabolic imbalances.
- Inadequate protein intake and malnutrition, along with age-related changes in appetite and metabolism, can contribute to muscle wasting and sarcopenia [28].
- Sedentary lifestyles and reduced physical activity levels are associated with muscle atrophy and an increased risk of sarcopenia [29].
- Certain chronic conditions, such as diabetes, chronic obstructive pulmonary disease, and inflammatory diseases, can contribute to sarcopenia through inflammatory processes, reduced physical activity, and impaired muscle metabolism [30].
Pathophysiology of sarcopenia
1) Aging
2) Hormonal changes
3) Nutritional factors
4) Physical inactivity
5) Chronic medical conditions
- Sarcopenia has significant implications for the health and well-being of affected individuals, as well as for healthcare systems and society as a whole. This section will discuss the main consequences of sarcopenia, including physical disability, fall risk and fractures, reduced QoL, and increased healthcare costs.
- 1. Physical disability
- The decline in muscle mass, strength, and function associated with sarcopenia can lead to impaired mobility and an increased risk of physical disability [3]. Everyday activities, such as walking, climbing stairs, and carrying objects, can become increasingly challenging for individuals with sarcopenia. As a result, affected individuals may experience a loss of independence and an increased reliance on assistance for daily tasks [31-33].
- 2. Risk of falls and fractures
- Sarcopenia is a significant risk factor for falls and fractures among older adults [34-36]. The decline in muscle strength and function can lead to impaired balance, coordination, and postural stability, which, in turn, increases the risk of falls. In a study conducted by Kinoshita et al. [37] in a Japanese population, sarcopenia was found to increase the odds ratio by 2.94 times in elderly patients, and a meta-analysis also suggested a significant causal relationship [38]. Falls are a leading cause of injury and disability in older adults, and fractures resulting from falls can have severe consequences, including long-term pain, disability, and increased mortality [9,39].
- 3. Quality of life
- Sarcopenia can negatively impact an individual’s QoL in various ways [3]. Physical limitations, loss of independence, and the increased risk of falls and fractures can contribute to reduced psychological well-being, social isolation, and depression [40-42]. Moreover, individuals with sarcopenia may experience fatigue, reduced stamina, and a decreased ability to engage in recreational activities, further diminishing their QoL [43].
- 4. Economic burden of healthcare
- Sarcopenia is associated with significant healthcare costs due to increased rates of hospitalization, rehabilitation, and long-term care [44]. The direct costs of managing sarcopenia-related complications, such as falls and fractures, as well as the indirect costs related to disability and loss of productivity, place a considerable burden on healthcare systems and society. With the growing prevalence of sarcopenia due to an aging global population, these costs are expected to rise in the coming years [7,8].
- 5. Miscellaneous
- Some systematic reviews and meta-analyses in the field of hepatology reported adverse outcomes of sarcopenia. Chang et al. [45] showed that sarcopenia was associated with increased mortality and tumor recurrence in patients with hepatocellular carcinoma, and another study reported that sarcopenia was significantly associated with hepatic encephalopathy in patients with cirrhosis [46]. Meanwhile, sarcopenia also affects the muscles involved in swallowing, causing sarcopenic dysphagia [47]. Dysphagia leads to malnutrition, creating a vicious cycle [48]. Although there are no golden diagnostic criteria for this condition, it can be diagnosed using a number of tools, including swallowing tests, video-fluoroscopic swallow study and surface electromyography, and ultrasound [47].
Adverse consequences of sarcopenia
- Early diagnosis and assessment of sarcopenia are crucial for implementing appropriate interventions and mitigating the associated health risks. An understanding of the criteria, tools, and methods used to diagnose sarcopenia through clinical and functional assessments used to evaluate the severity and impact of the patient's condition is essential.
- 1. Diagnostic tools
- Various tools and methods have been developed for diagnosing sarcopenia, which typically involve the assessment of muscle mass, strength, and function. In large epidemiologic surveys in the community, anthropometric measurements can be used to estimate muscle mass and body composition and to screen for sarcopenia, as testing with equipment can be difficult [5]. There have been, and continue to be, many studies to find noninvasive and safe methods. The most optimal methods used to measure muscle volume are magnetic resonance or computed tomography. However, these tests are expensive and no cutoff value has been established to date, so dual-energy X-ray absorptiometry (DXA) or bioelectrical impedance analysis (BIA) is used [49]. Common diagnostic tools and methods are as follows.
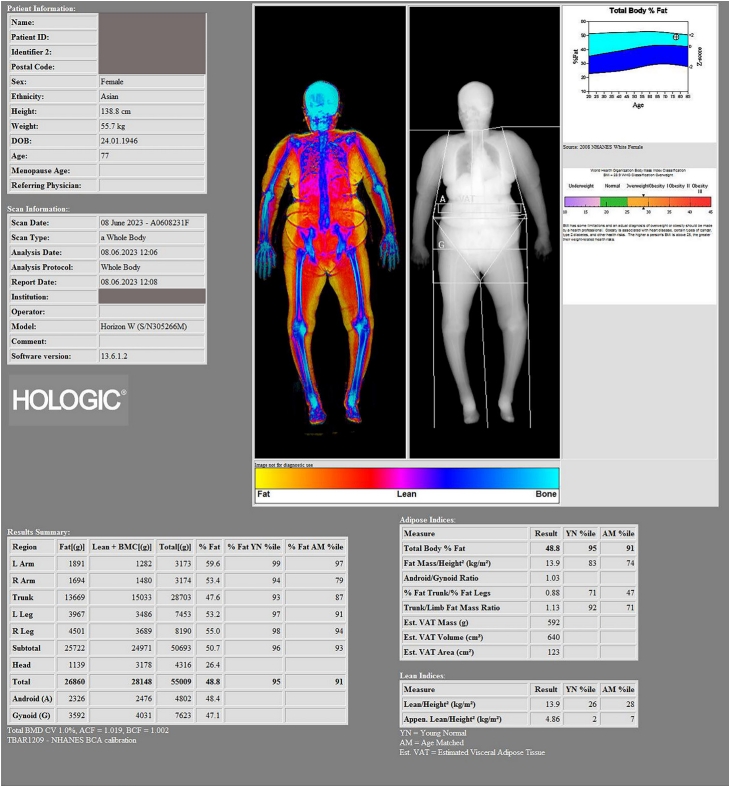
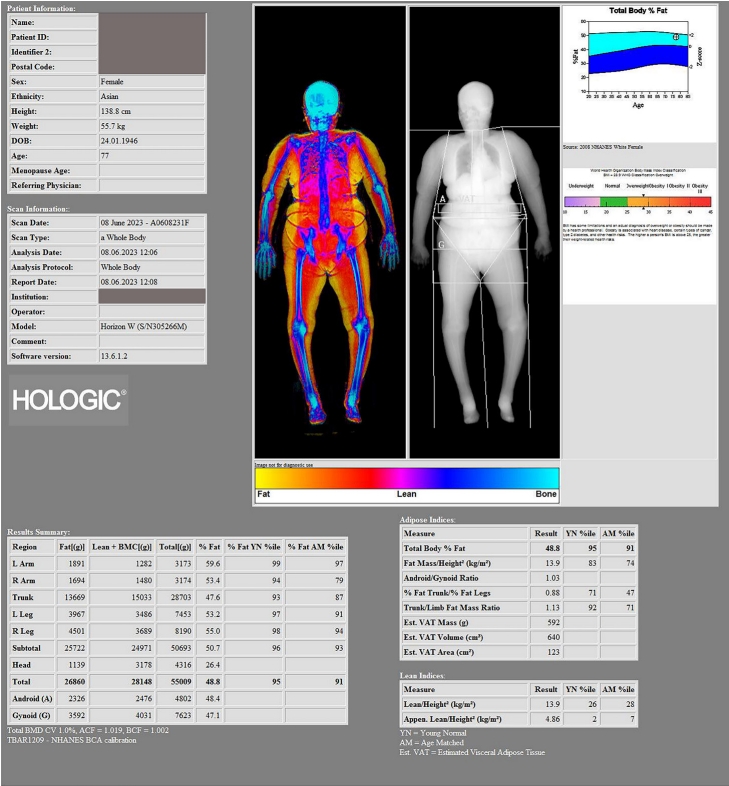
- DXA is a widely used technique for assessing muscle mass and body composition. It is considered the gold standard for diagnosing sarcopenia due to its accuracy, precision, and low radiation exposure. Methods for estimating muscle mass using DXA are not yet fully established. However, the European Working Group on Sarcopenia in Older People-2 (EWGSOP-2) suggests cutoff values for estimating muscle mass using DXA: appendicular lean (skeletal) mass or appendicular lean (skeletal) mass index (appendicular lean mass/height2) (Fig. 1). For appendicular lean mass, it is recommended to define <15 kg/m2 for women and <20 kg/m2 for men, while appendicular lean mass index is defined as <5.5 kg/m2 for women and <7.0 kg/m2 for men [3,50,51].
- BIA is a noninvasive method for estimating muscle mass and body composition based on the electrical properties of tissues. BIA uses electrical conductivity throughout the body to indirectly calculate muscle mass [52]. It is recommended to consider the measurements using the cross-validated Sergi equation [53], as the measurements may vary from one device to another, and there may be differences based on the population used. It also has the disadvantage that the amount of water in the body can affect the measurement. However, it is a more accessible and affordable alternative to DXA, although it may be less accurate in some cases [54].
- Muscle strength was assessed with a handgrip strength test using a dynamometer or a vigorimeter. A dynamometer is used to measure isometric handgrip strength [55]. Measurements are given in kilograms. The correct posture for measurement is seated, shoulders adducted and neutrally rotated, elbow flexed 90°, forearm in a neutral position, wrist in dorsiflexion 0° to 30°, ulnar deviation 0° to 15°, avoiding overlap with other motor tasks [55,56]. A vigorimeter is measured by the patient contracting a kind of rubber ball connected to a manometer. The maximum pressure achieved by this ball corresponds to the maximum handgrip strength and is expressed in kilopascals. The use of different ball sizes makes it possible to adapt to different hand sizes, thus ensuring uniform muscle tension [55,57]. Handgrip strength is a relatively simple, cost-effective, and reliable measure of overall muscle strength. It is commonly assessed using a handheld dynamometer and has been shown to be a strong predictor of sarcopenia and related health outcomes [58]. The EWGSOP-2 defined the cutoff value for grip strength as <27 kg for men and <16 kg for women (Fig. 2) [3].
- Gait or walking speed is widely used for assessing the functional performance of sarcopenia. A slow gait speed has been associated with an increased risk of sarcopenia, disability, and adverse health outcomes. A commonly used walking speed test is called the 6-meter usual walking speed test, which uses a stopwatch or electronic device to measure the gait timing [59]. Generally, low functional performance was defined as a gait speed of <1.0 m/sec for both men and women [3].
- 2. Diagnostic criteria
- Sarcopenia, the age-related loss of muscle mass, strength, and function, has been increasingly recognized as a significant public health concern. The diagnostic criteria for sarcopenia vary, with differences noted particularly between Europe and Asia (Table 1).
- For Europe, the EWGSOP proposed diagnostic criteria in 2010, which were later revised in 2019 (EWGSOP-2). In their updated criteria, sarcopenia is recognized primarily by a reduction in muscle strength and confirmed by either a reduction in muscle quantity or quality. Severe sarcopenia, according to the EWGSOP-2, is identified by the presence of low muscle quantity, quality, and physical performance [3].
- In contrast, in Asia, the Asian Working Group for Sarcopenia (AWGS) suggested different cutoff points considering the different body compositions and lifestyles compared to Western populations. Low muscle mass was defined as an appendicular skeletal muscle index of <5.4 kg/m2 for women and <7.0 kg/m2 for men. The AWGS also recommended using muscle strength and physical performance to diagnose sarcopenia, but the cutoff points for muscle mass, grip strength, and gait speed are lower than those suggested by the EWGSOP [33].
- 3. Other tools for clinical and functional assessments
- In addition to the diagnostic tools and methods for sarcopenia, various clinical and functional assessments can be used to evaluate the severity and impact of sarcopenia on an individual’s health and well-being.
- The short physical performance battery (SPPB) is a widely used assessment tool that evaluates lower extremity function through a series of the balance test, the usual gait speed, and the repeated chair stands test [60]. It is a strong predictor of disability, falls, and mortality in older adults [61]. The balance test requires the subject to maintain three increasingly difficult positions: a side-by-side, semi-tandem (standing with the heel of one foot next to the big toe of the other), and tandem (touching with the heel of one foot in front of the toe of the other) for 10 seconds each. The balance test is scored based on the total time a subject holds each position (from 0 to 30 seconds) [60]. The subject is asked to walk a 4-meter course at their usual walking speed [62]. The subject is instructed to stand with both feet touching the starting line and then to start walking. They may use a walking aid (cane, walker, or other walking aid) if necessary, but may not be assisted by another person. When the start signal is given, timing begins and the number of seconds required to complete the full distance is recorded. The faster of the two steps is then used to calculate the SPPB score. The repeated chair stands test is performed with the back against a wall using a straight-backed chair. The subject is first asked to stand up from a sitting position without using their arms. If they are able to do this, they are asked to repeat the standing and sitting movement as quickly as possible, crossing their arms over their chest five times. The time taken to complete five stands is then recorded [62].
- The Timed Up and Go test measures the time it takes for an individual to stand up from a chair, walk a short distance, turn around, and return to the chair. It is a simple and reliable assessment of mobility, balance, and functional status [63,64].
- This test evaluates lower body strength by measuring the number of times an individual can stand up from a seated position within 30 seconds. It is a useful predictor of functional performance, falls, and disability in older adults [65,66].
Diagnosis and assessment of sarcopenia
1) Dual-energy X-ray absorptiometry
2) Bioelectrical impedance analysis
3) Handgrip strength
4) Gait speed
1) Short physical performance battery
2) Timed Up and Go test
3) Thirty-second chair stand test
- Effective management strategies for sarcopenia focus on addressing the underlying causes and mitigating the consequences of the condition. Therefore, a multidisciplinary approach is needed to manage sarcopenia, including exercise interventions, nutritional interventions, and pharmacological interventions.
- 1. Exercise interventions
- Physical activity, particularly resistance training, is considered the cornerstone of sarcopenia management. Exercise interventions can help maintain and build muscle mass, strength, and function, as well as improve overall health and well-being. Key components of exercise interventions for sarcopenia include as follows.
- It involves working against external resistance (e.g., free weights, resistance bands, or body weight) and has been shown to be effective in increasing muscle mass, strength, and function in older adults [67]. It is recommended that older adults engage in resistance training at least 2 to 3 times per week, targeting all major muscle groups [68].
- Aerobic exercise such as walking, cycling, or swimming, can help improve cardiovascular health, endurance, and overall functional capacity in older adults [69]. It is recommended that older adults engage in moderate-intensity aerobic exercise for at least 150 minutes per week [70].
- Incorporating balance and flexibility exercises into an exercise program can help improve postural stability, reduce fall risk, and maintain functional mobility in older adults [71,72].
- A randomized controlled trial demonstrated the effectiveness of early exercise and nutritional intervention in sarcopenic elders [73]. It was reported that early exercise and nutritional intervention may help in the early recovery of lower limb muscle mass in sarcopenic elders. In particular, the authors suggested that when planning a rehabilitation program for patients with sarcopenia, resistance training with nutritional support may be beneficial for rapid gains in muscle mass.
- 2. Nutritional interventions
- Proper nutrition is essential for maintaining muscle mass and function, and nutritional interventions can play a critical role in the management of sarcopenia. Key nutritional strategies for sarcopenia are as follows.
- Ensuring adequate protein intake is crucial for maintaining and building muscle mass [74]. Older adults should aim for a daily protein intake of at least 1.0 to 1.2 g per kg of body weight, with an emphasis on high-quality protein sources, such as lean meats, poultry, fish, dairy, and plant-based options [75].
- Muscle loss is caused by an imbalance between the anabolic and catabolic processes of protein. Amino acids are the main building blocks for muscle synthesis. In particular, branched-chain amino acids (BCAAs) regulate the mammalian target of rapamycin (mTOR) process in protein synthesis [76-78]. Recent studies have focused on reduced skeletal muscle sensitivity to amino acids as a potential mechanism of sarcopenia. Guillet et al. [79] suggested that defective activation of the BCAA pathway may be an important contributor to sarcopenia. In animal studies, administration of leucine can stimulate the rate of muscle protein synthesis [80,81]. Accordingly, BCAA administration may be beneficial in reversing age-related protein loss. Based on these findings, there has been a lot of interest in developing drugs for sarcopenia using BCAAs.
- Adequate vitamin D and calcium intake are important for bone health and may also play a role in maintaining muscle function [82]. Supplementation may be necessary for older adults who are deficient in these nutrients.
- Maintaining an appropriate energy balance is important for preventing muscle wasting and supporting muscle growth. Older adults should consume a balanced diet with sufficient calories to meet their energy needs and support their exercise interventions [83,84].
- 3. Pharmacological interventions
- Pharmacological interventions for sarcopenia are still in the early stage of development, and further research is needed to determine their efficacy and safety. Some potential pharmacological treatments for sarcopenia include the following.
- Testosterone replacement therapy in men and hormone replacement therapy in postmenopausal women may help improve muscle mass and strength. However, these therapies carry potential risks and should be carefully considered on an individual basis [85,86].
- Myostatin is a protein that regulates muscle growth, and inhibiting its action has been shown to promote muscle growth in preclinical studies [87,88]. Further research is needed to determine the effectiveness and safety of myostatin inhibitors in the treatment of sarcopenia.
- Selective androgen receptor modulators (SARMs) are a class of drugs that selectively target androgen receptors, promoting muscle growth without the adverse effects associated with traditional anabolic steroids. Clinical trials are ongoing to evaluate the potential of SARMs as a treatment for sarcopenia [89].
Multidisciplinary approach for sarcopenia
1) Resistance training
2) Aerobic exercise
3) Balance and flexibility training
1) Protein intake
2) Branched amino acids (valine, leucine, and isoleucine)
3) Vitamin D and calcium
4) Energy balance
1) Hormone replacement therapy
2) Myostatin inhibitors
3) Selective androgen receptor modulators
- As the global population continues to age, the prevalence of sarcopenia and its associated health risks is expected to increase [7]. This growing public health concern underscores the need for continued research and innovation in the prevention, diagnosis, and management of sarcopenia. This section will discuss future directions and research priorities in the field of sarcopenia, including the development of novel biomarkers, new pharmacological interventions.
- 1. Novel biomarkers for sarcopenia
- The identification of reliable and easily accessible biomarkers for sarcopenia can significantly improve early diagnosis and facilitate the development of targeted interventions. Future research should focus on discovering and validating novel biomarkers, such as blood-based markers, genetic factors, or imaging-based parameters, that can help predict the risk, progression, and response to treatment in sarcopenia. In their study, Furutani et al. [90] combined messenger RNA analysis from mononuclear cells in serum with clinical information to create a model with high diagnostic sensitivity. There have also been studies that have attempted to use circulating microRNAs (miRNAs) as biomarkers. A meta-analysis of these studies suggests that miRNAs also have potential value as biomarkers with further research [91].
- Recently, researchers have been focusing on extracellular vesicles (EVs) to demonstrate the paracrine effects of stem cells. The advantage of EVs is that they have a cargo that includes the properties of the originating cells, and they are ubiquitous in the body’s fluids and can be obtained relatively noninvasively. The study of EVs in relation to sarcopenia is also ongoing, and research has shown that EVs may be one of the underlying mechanisms of sarcopenia and can be used as a biomarker [92].
- 2. New screening test for sarcopenia
- Although DXA is a noninvasive and relatively widely used diagnostic method for sarcopenia, it has the disadvantage of requiring equipment and cost. Recently, a study was conducted to develop a screening tool using the rapidly growing field of artificial intelligence (AI) models, and the authors claimed to have developed a model with a similar level of accuracy to DXA using physical measurements [93]. In fact, this approach is being tried in many areas of medicine, and diagnosis using models trained through trial and error is valuable as a low-cost and relatively accurate screening tool. Zupo et al. [94] developed an optimized model for screening for sarcopenia using machine learning with various anthropometric measurements and biological markers. With further research, we may see AI diagnostics as a diagnostic tool in the not-too-distant future.
- 3. New pharmacological interventions
- The development of pharmacological interventions for sarcopenia represents an emerging and rapidly evolving field of research. While potential candidates like hormone replacement therapies, myostatin inhibitors, and SARMs have shown promise in preliminary studies, their application in clinical practice remains limited due to concerns over safety, side effects, and the need for further validation of efficacy. Hormone replacement therapies, for instance, may enhance muscle mass and strength, but they also carry risks that necessitate careful individualized consideration. Myostatin inhibitors, which counteract a protein that regulates muscle growth, have demonstrated positive outcomes in preclinical studies, yet their effectiveness and safety in the treatment of sarcopenia require further investigation [95]. Therefore, many myostatin inhibitors are currently undergoing clinical trials to confirm their safety and effectiveness [96]. SARMs, which selectively target androgen receptors to promote muscle growth without the adverse effects associated with traditional anabolic steroids, are currently under clinical trial evaluation [97]. As the global aging population continues to rise, and with it the prevalence of sarcopenia, the demand for effective pharmacological treatments will only become more pressing. Therefore, continued investment in comprehensive research and rigorous clinical trials is crucial to progress in this area.
Novel diagnostic tools and developments in sarcopenia
- Sarcopenia, characterized by the age-related decline in muscle mass, strength, and function, is a growing public health concern due to the increasing global aging population. It is associated with numerous adverse health outcomes.
- The implications for the future include: (1) Continued efforts to raise public awareness and understanding of sarcopenia, emphasizing the importance of early detection, intervention, and prevention measures. (2) Advancements in the development of novel diagnostic tools and biomarkers that facilitate early identification and targeted interventions for sarcopenia. (3) Continued research and innovation in the field of sarcopenia, focusing on the development of new pharmacological treatments, the identification of genetic and epigenetic factors, and personalized approaches to care. (4) Integration of multi- and interdisciplinary collaboration in the prevention, diagnosis, and management of sarcopenia, ensuring a comprehensive and individualized approach to care. (5) Implementation of effective public health policies and programs that support research, innovation, and community-based initiatives aimed at preventing and managing sarcopenia.
Concluding remarks and perspectives
- Addressing the challenges posed by sarcopenia requires a multidisciplinary approach that encompasses research, healthcare, and public health initiatives. By enhancing our understanding of sarcopenia and implementing evidence-based strategies for prevention, diagnosis, and management, we can work towards improving the health, mobility, and QoL of older adults worldwide.
Conclusion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2021R1A6A1A03040177).
-
Author contributions
Conceptualization: all authors; Data curation, Project administration: GBK; Formal analysis, Supervision: OJS; Funding acquisition, Validation: WTP, GBK; Methodology: WTP; Resources: OJS, GBK; Writing-original draft: WTP, GBK; Writing-review & editing: WTP, OJS.
Notes

| Diagnostic criteria | EWGSOP-2 (Europe) [3] | AWGS 2019 (Asia) [33] |
|---|---|---|
| Low muscle strength by handgrip | Men <27.0 kg, women <16.0 kg | Men <28.0 kg, women <18.0 kg |
| Low muscle mass (ASM indexa)) by DXA | Men <7.0 kg/m², women <5.5 kg/m² | Men <7.0 kg/m², women <5.4 kg/m² |
| Decreased physical performance | Gait speed <0.8 m/secb), SPPB ≤8, TUG ≥20 sec | Gait speed <1.0 m/secb), SPPB ≤9, |
| 5-time chair stand test ≥12 sec |
EWGSOP-2, European Working Group on Sarcopenia in Older People-2; AWGS, Asian Working Group for Sarcopenia; ASM, appendicular skeletal muscle mass; DXA, dual-energy X-ray absorptiometry; SPPB, short physical performance battery; TUG, Timed Up and Go test.
a) ASM index was calculated as ASM/height2 measured by DXA.
b) Gait speed measured by 6-meter walking speed test.
- 1. Evans WJ. Sarcopenia should reflect the contribution of age-associated changes in skeletal muscle to risk of morbidity and mortality in elderly people. J Am Med Dir Assoc 2015;16:546–7.ArticlePubMed
- 2. Volpi E, Nazemi R, Fujita S. Muscle tissue changes with aging. Curr Opin Clin Nutr Metab Care 2004;7:405–10.ArticlePubMedPMC
- 3. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019;48:16–31.ArticlePubMedPDF
- 4. Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr 1997;127:990S–1S.ArticlePubMed
- 5. Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998;147:755–63.ArticlePubMed
- 6. Shon OJ, Kim GB, Cho SJ. Does sarcopenia accompanying end-stage knee osteoarthritis affect the outcomes following total knee arthroplasty? Medicina (Kaunas) 2023;59:1078.ArticlePubMedPMC
- 7. Shafiee G, Keshtkar A, Soltani A, Ahadi Z, Larijani B, Heshmat R. Prevalence of sarcopenia in the world: a systematic review and meta-analysis of general population studies. J Diabetes Metab Disord 2017;16:21.ArticlePubMedPMCPDF
- 8. Bruyère O, Beaudart C, Ethgen O, Reginster JY, Locquet M. The health economics burden of sarcopenia: a systematic review. Maturitas 2019;119:61–9.ArticlePubMed
- 9. Beaudart C, Rizzoli R, Bruyère O, Reginster JY, Biver E. Sarcopenia: burden and challenges for public health. Arch Public Health 2014;72:45.ArticlePubMedPMCPDF
- 10. Abate M, Di Iorio A, Di Renzo D, Paganelli R, Saggini R, Abate G. Frailty in the elderly: the physical dimension. Eura Medicophys 2007;43:407–15.PubMed
- 11. Faulkner JA, Larkin LM, Claflin DR, Brooks SV. Age-related changes in the structure and function of skeletal muscles. Clin Exp Pharmacol Physiol 2007;34:1091–6.ArticlePubMed
- 12. Ryall JG, Schertzer JD, Lynch GS. Cellular and molecular mechanisms underlying age-related skeletal muscle wasting and weakness. Biogerontology 2008;9:213–28.ArticlePubMedPDF
- 13. Melton LJ, Khosla S, Crowson CS, O'Connor MK, O'Fallon WM, Riggs BL. Epidemiology of sarcopenia. J Am Geriatr Soc 2000;48:625–30.ArticlePubMed
- 14. Cermak NM, Snijders T, McKay BR, Parise G, Verdijk LB, Tarnopolsky MA, et al. Eccentric exercise increases satellite cell content in type II muscle fibers. Med Sci Sports Exerc 2013;45:230–7.ArticlePubMed
- 15. Nguyen MK, Kurtz I. Quantitative interrelationship between Gibbs-Donnan equilibrium, osmolality of body fluid compartments, and plasma water sodium concentration. J Appl Physiol (1985) 2006;100:1293–300.ArticlePubMed
- 16. Narici MV, Maffulli N. Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull 2010;95:139–59.ArticlePubMed
- 17. Larsson L, Degens H, Li M, Salviati L, Lee YI, Thompson W, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev 2019;99:427–511.ArticlePubMed
- 18. Power GA, Dalton BH, Rice CL. Human neuromuscular structure and function in old age: a brief review. J Sport Health Sci 2013;2:215–26.ArticlePubMed
- 19. Coppi E, Houdayer E, Chieffo R, Spagnolo F, Inuggi A, Straffi L, et al. Age-related changes in motor cortical representation and interhemispheric interactions: a transcranial magnetic stimulation study. Front Aging Neurosci 2014;6:209.ArticlePubMedPMC
- 20. Clanton TL. Hypoxia-induced reactive oxygen species formation in skeletal muscle. J Appl Physiol (1985) 2007;102:2379–88.ArticlePubMed
- 21. Snijders T, Nederveen JP, McKay BR, Joanisse S, Verdijk LB, van Loon LJ, et al. Satellite cells in human skeletal muscle plasticity. Front Physiol 2015;6:283.ArticlePubMedPMC
- 22. Basualto-Alarcón C, Varela D, Duran J, Maass R, Estrada M. Sarcopenia and androgens: a link between pathology and treatment. Front Endocrinol (Lausanne) 2014;5:217.ArticlePubMedPMC
- 23. McDonald VM, Simpson JL, Higgins I, Gibson PG. Multidimensional assessment of older people with asthma and COPD: clinical management and health status. Age Ageing 2011;40:42–9.ArticlePubMed
- 24. Ferrando AA, Sheffield-Moore M, Paddon-Jones D, Wolfe RR, Urban RJ. Differential anabolic effects of testosterone and amino acid feeding in older men. J Clin Endocrinol Metab 2003;88:358–62.ArticlePubMed
- 25. Messier V, Rabasa-Lhoret R, Barbat-Artigas S, Elisha B, Karelis AD, Aubertin-Leheudre M. Menopause and sarcopenia: a potential role for sex hormones. Maturitas 2011;68:331–6.ArticlePubMed
- 26. Santini MP, Tsao L, Monassier L, Theodoropoulos C, Carter J, Lara-Pezzi E, et al. Enhancing repair of the mammalian heart. Circ Res 2007;100:1732–40.ArticlePubMedPMC
- 27. Fitts RH, Romatowski JG, Peters JR, Paddon-Jones D, Wolfe RR, Ferrando AA. The deleterious effects of bed rest on human skeletal muscle fibers are exacerbated by hypercortisolemia and ameliorated by dietary supplementation. Am J Physiol Cell Physiol 2007;293:C313–20.ArticlePubMed
- 28. Paddon-Jones D, Rasmussen BB. Dietary protein recommendations and the prevention of sarcopenia. Curr Opin Clin Nutr Metab Care 2009;12:86–90.ArticlePubMedPMC
- 29. Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A, Orlandini A, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015;386:266–73.ArticlePubMed
- 30. Morley JE, Anker SD, von Haehling S. Prevalence, incidence, and clinical impact of sarcopenia: facts, numbers, and epidemiology-update 2014. J Cachexia Sarcopenia Muscle 2014;5:253–9.ArticlePubMedPMC
- 31. Cruz-Jentoft AJ, Landi F, Schneider SM, Zúñiga C, Arai H, Boirie Y, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014;43:748–59.ArticlePubMedPMC
- 32. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet 2019;393:2636–46.ArticlePubMed
- 33. Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2014;15:95–101.ArticlePubMed
- 34. Szulc P, Beck TJ, Marchand F, Delmas PD. Low skeletal muscle mass is associated with poor structural parameters of bone and impaired balance in elderly men: the MINOS study. J Bone Miner Res 2005;20:721–9.ArticlePubMed
- 35. Edwards MH, Gregson CL, Patel HP, Jameson KA, Harvey NC, Sayer AA, et al. Muscle size, strength, and physical performance and their associations with bone structure in the Hertfordshire Cohort Study. J Bone Miner Res 2013;28:2295–304.ArticlePubMed
- 36. Sjöblom S, Suuronen J, Rikkonen T, Honkanen R, Kröger H, Sirola J. Relationship between postmenopausal osteoporosis and the components of clinical sarcopenia. Maturitas 2013;75:175–80.ArticlePubMed
- 37. Kinoshita K, Satake S, Matsui Y, Arai H. Association between sarcopenia and fall risk according to the muscle mass adjustment method in Japanese older outpatients. J Nutr Health Aging 2021;25:762–6.ArticlePubMedPDF
- 38. Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J Am Geriatr Soc 2004;52:1121–9.ArticlePubMed
- 39. Álvarez-Barbosa F, del Pozo-Cruz J, del Pozo-Cruz B, Alfonso-Rosa RM, Rogers ME, Zhang Y. Effects of supervised whole body vibration exercise on fall risk factors, functional dependence and health-related quality of life in nursing home residents aged 80+. Maturitas 2014;79:456–63.ArticlePubMed
- 40. Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, et al. Frailty consensus: a call to action. J Am Med Dir Assoc 2013;14:392–7.ArticlePubMedPMC
- 41. Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing 2006;35:ii37–41.ArticlePubMed
- 42. Beaudart C, Biver E, Bruyère O, Cooper C, Al-Daghri N, Reginster JY, et al. Quality of life assessment in musculo-skeletal health. Aging Clin Exp Res 2018;30:413–8.ArticlePubMedPDF
- 43. Ethgen O, Beaudart C, Buckinx F, Bruyère O, Reginster JY. The future prevalence of sarcopenia in Europe: a claim for public health action. Calcif Tissue Int 2017;100:229–34.ArticlePubMedPDF
- 44. Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc 2004;52:80–5.ArticlePubMed
- 45. Chang KV, Chen JD, Wu WT, Huang KC, Hsu CT, Han DS. Association between loss of skeletal muscle mass and mortality and tumor recurrence in hepatocellular carcinoma: a systematic review and meta-analysis. Liver Cancer 2018;7:90–103.ArticlePubMedPDF
- 46. Chang KV, Chen JD, Wu WT, Huang KC, Lin HY, Han DS. Is sarcopenia associated with hepatic encephalopathy in liver cirrhosis? A systematic review and meta-analysis. J Formos Med Assoc 2019;118:833–42.ArticlePubMed
- 47. Chen KC, Jeng Y, Wu WT, Wang TG, Han DS, Özçakar L, et al. Sarcopenic dysphagia: a narrative review from diagnosis to intervention. Nutrients 2021;13:4043.ArticlePubMedPMC
- 48. Nishioka S, Okamoto T, Takayama M, Urushihara M, Watanabe M, Kiriya Y, et al. Malnutrition risk predicts recovery of full oral intake among older adult stroke patients undergoing enteral nutrition: secondary analysis of a multicentre survey (the APPLE study). Clin Nutr 2017;36:1089–96.ArticlePubMed
- 49. Setiati S. Diagnostic tools for sarcopenia: can we get less expensive and accurate methods? Acta Med Indones 2019;51:93–4.PubMed
- 50. Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci 2014;69:547–58.ArticlePubMedPMC
- 51. Gould H, Brennan SL, Kotowicz MA, Nicholson GC, Pasco JA. Total and appendicular lean mass reference ranges for Australian men and women: the Geelong osteoporosis study. Calcif Tissue Int 2014;94:363–72.ArticlePubMedPDF
- 52. Lukaski HC. Evolution of bioimpedance: a circuitous journey from estimation of physiological function to assessment of body composition and a return to clinical research. Eur J Clin Nutr 2013;67(Suppl 1):S2–9.ArticlePubMedPDF
- 53. Sergi G, De Rui M, Veronese N, Bolzetta F, Berton L, Carraro S, et al. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin Nutr 2015;34:667–73.ArticlePubMed
- 54. Yu SC, Powell A, Khow KS, Visvanathan R. The performance of five bioelectrical impedance analysis prediction equations against dual X-ray absorptiometry in estimating appendicular skeletal muscle mass in an adult Australian population. Nutrients 2016;8:189.ArticlePubMedPMC
- 55. Baek JY, Jung HW, Kim KM, Kim M, Park CY, Lee KP, et al. Korean Working Group on Sarcopenia guideline: expert consensus on sarcopenia screening and diagnosis by the Korean Society of Sarcopenia, the Korean Society for Bone and Mineral Research, and the Korean Geriatrics Society. Ann Geriatr Med Res 2023;27:9–21.ArticlePubMedPMCPDF
- 56. Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S. Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil 1985;66:69–74.PubMed
- 57. Desrosiers J, Hébert R, Bravo G, Dutil E. Comparison of the Jamar dynamometer and the Martin vigorimeter for grip strength measurements in a healthy elderly population. Scand J Rehabil Med 1995;27:137–43.ArticlePubMedPDF
- 58. Dodds RM, Syddall HE, Cooper R, Benzeval M, Deary IJ, Dennison EM, et al. Grip strength across the life course: normative data from twelve British studies. PLoS One 2014;9:e113637.ArticlePubMedPMC
- 59. Maggio M, Ceda GP, Ticinesi A, De Vita F, Gelmini G, Costantino C, et al. Instrumental and non-instrumental evaluation of 4-meter walking speed in older individuals. PLoS One 2016;11:e0153583.ArticlePubMedPMC
- 60. Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 1994;49(Suppl 2):M85–94.ArticlePubMed
- 61. Pavasini R, Guralnik J, Brown JC, di Bari M, Cesari M, Landi F, et al. Short Physical Performance Battery and all-cause mortality: systematic review and meta-analysis. BMC Med 2016;14:215.ArticlePubMedPMCPDF
- 62. Gill TM. Assessment of function and disability in longitudinal studies. J Am Geriatr Soc 2010;58(Suppl 2):S308–12.ArticlePubMedPMC
- 63. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142–8.ArticlePubMed
- 64. Barry E, Galvin R, Keogh C, Horgan F, Fahey T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: a systematic review and meta-analysis. BMC Geriatr 2014;14:14.ArticlePubMedPMCPDF
- 65. Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport 1999;70:113–9.ArticlePubMed
- 66. Bohannon RW. Sit-to-stand test for measuring performance of lower extremity muscles. Percept Mot Skills 1995;80:163–6.ArticlePubMedPDF
- 67. Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD, et al. Resistance training for older adults: position statement from the National Strength and Conditioning Association. J Strength Cond Res 2019;33:2019–52.ArticlePubMed
- 68. Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C, Feigenbaum MS, et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc 2002;34:364–80.ArticlePubMed
- 69. Loprinzi PD, Lee H, Cardinal BJ. Evidence to support including lifestyle light-intensity recommendations in physical activity guidelines for older adults. Am J Health Promot 2015;29:277–84.ArticlePubMedPDF
- 70. Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA 2018;320:2020–8.ArticlePubMedPMC
- 71. Granacher U, Gollhofer A, Hortobágyi T, Kressig RW, Muehlbauer T. The importance of trunk muscle strength for balance, functional performance, and fall prevention in seniors: a systematic review. Sports Med 2013;43:627–41.ArticlePubMedPDF
- 72. Page P. Current concepts in muscle stretching for exercise and rehabilitation. Int J Sports Phys Ther 2012;7:109–19.PubMedPMC
- 73. Chang KV, Wu WT, Huang KC, Han DS. Effectiveness of early versus delayed exercise and nutritional intervention on segmental body composition of sarcopenic elders: a randomized controlled trial. Clin Nutr 2021;40:1052–9.ArticlePubMed
- 74. Bauer J, Biolo G, Cederholm T, Cesari M, Cruz-Jentoft AJ, Morley JE, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc 2013;14:542–59.ArticlePubMed
- 75. Houston DK, Nicklas BJ, Ding J, Harris TB, Tylavsky FA, Newman AB, et al. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: the Health, Aging, and Body Composition (Health ABC) Study. Am J Clin Nutr 2008;87:150–5.ArticlePubMed
- 76. Wolfe RR. The underappreciated role of muscle in health and disease. Am J Clin Nutr 2006;84:475–82.ArticlePubMed
- 77. Rennie MJ, Tipton KD. Protein and amino acid metabolism during and after exercise and the effects of nutrition. Annu Rev Nutr 2000;20:457–83.ArticlePubMed
- 78. Norton LE, Layman DK. Leucine regulates translation initiation of protein synthesis in skeletal muscle after exercise. J Nutr 2006;136:533S–7S.ArticlePubMed
- 79. Guillet C, Prod’homme M, Balage M, Gachon P, Giraudet C, Morin L, et al. Impaired anabolic response of muscle protein synthesis is associated with S6K1 dysregulation in elderly humans. FASEB J 2004;18:1586–7.ArticlePubMedPDF
- 80. Rieu I, Balage M, Sornet C, Debras E, Ripes S, Rochon-Bonhomme C, et al. Increased availability of leucine with leucine-rich whey proteins improves postprandial muscle protein synthesis in aging rats. Nutrition 2007;23:323–31.ArticlePubMed
- 81. Rieu I, Balage M, Sornet C, Giraudet C, Pujos E, Grizard J, et al. Leucine supplementation improves muscle protein synthesis in elderly men independently of hyperaminoacidaemia. J Physiol 2006;575:305–15.ArticlePubMedPMC
- 82. Beaudart C, Buckinx F, Rabenda V, Gillain S, Cavalier E, Slomian J, et al. The effects of vitamin D on skeletal muscle strength, muscle mass, and muscle power: a systematic review and meta-analysis of randomized controlled trials. J Clin Endocrinol Metab 2014;99:4336–45.ArticlePubMed
- 83. Deutz NE, Bauer JM, Barazzoni R, Biolo G, Boirie Y, Bosy-Westphal A, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clin Nutr 2014;33:929–36.ArticlePubMedPMC
- 84. Phillips SM. Nutritional supplements in support of resistance exercise to counter age-related sarcopenia. Adv Nutr 2015;6:452–60.ArticlePubMedPMC
- 85. Srinivas-Shankar U, Roberts SA, Connolly MJ, O’Connell MD, Adams JE, Oldham JA, et al. Effects of testosterone on muscle strength, physical function, body composition, and quality of life in intermediate-frail and frail elderly men: a randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab 2010;95:639–50.ArticlePubMed
- 86. Davis SR, Wahlin-Jacobsen S. Testosterone in women: the clinical significance. Lancet Diabetes Endocrinol 2015;3:980–92.ArticlePubMed
- 87. Morley JE. Pharmacologic options for the treatment of sarcopenia. Calcif Tissue Int 2016;98:319–33.ArticlePubMedPDF
- 88. Latres E, Amini AR, Amini AA, Griffiths J, Martin FJ, Wei Y, et al. Insulin-like growth factor-1 (IGF-1) inversely regulates atrophy-induced genes via the phosphatidylinositol 3-kinase/Akt/mammalian target of rapamycin (PI3K/Akt/mTOR) pathway. J Biol Chem 2005;280:2737–44.ArticlePubMed
- 89. Dalton JT, Barnette KG, Bohl CE, Hancock ML, Rodriguez D, Dodson ST, et al. The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women: results of a double-blind, placebo-controlled phase II trial. J Cachexia Sarcopenia Muscle 2011;2:153–61.ArticlePubMedPMCPDF
- 90. Furutani M, Suganuma M, Akiyama S, Mitsumori R, Takemura M, Matsui Y, et al. RNA-sequencing analysis identification of potential biomarkers for diagnosis of sarcopenia. J Gerontol A Biol Sci Med Sci 2023;Jun 22 [Epub] https://doi.org/10.1093/gerona/glad150.Article
- 91. Salamanna F, Contartese D, Ruffilli A, Barile F, Bellavia D, Marchese L, et al. Sharing circulating micro-RNAs between osteoporosis and sarcopenia: a systematic review. Life (Basel) 2023;13:602.ArticlePubMedPMC
- 92. Wang LX, Zhang X, Guan LJ, Pen Y. What role do extracellular vesicles play in developing physical frailty and sarcopenia?: a systematic review. Z Gerontol Geriatr 2022;Dec 2 [Epub]. https://doi.org/10.1007/s00391-022-02150-3.Article
- 93. Buccheri E, Dell'Aquila D, Russo M, Chiaramonte R, Musumeci G, Vecchio M. Can artificial intelligence simplify the screening of muscle mass loss? Heliyon 2023;9:e16323.ArticlePubMedPMC
- 94. Zupo R, Moroni A, Castellana F, Gasparri C, Catino F, Lampignano L, et al. A machine-learning approach to target clinical and biological features associated with sarcopenia: findings from northern and southern Italian aging populations. Metabolites 2023;13:565.ArticlePubMedPMC
- 95. Dao T, Green AE, Kim YA, Bae SJ, Ha KT, Gariani K, et al. Sarcopenia and muscle aging: a brief overview. Endocrinol Metab (Seoul) 2020;35:716–32.ArticlePubMedPMCPDF
- 96. Jang JY, Kim D, Kim ND. Pathogenesis, intervention, and current status of drug development for sarcopenia: a review. Biomedicines 2023;11:1635.ArticlePubMedPMC
- 97. Christiansen AR, Lipshultz LI, Hotaling JM, Pastuszak AW. Selective androgen receptor modulators: the future of androgen therapy? Transl Androl Urol 2020;9(Suppl 2):S135–48.ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite