- Skip Navigation
- Skip to contents
 E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 37(4); 2020 > Article
-
Focused Review article
Therapeutic potential of targeting kinase inhibition in patients with idiopathic pulmonary fibrosis -
Suji Kim1,2
 , Jae Hyang Lim3, Chang-Hoon Woo1,2
, Jae Hyang Lim3, Chang-Hoon Woo1,2 -
Yeungnam University Journal of Medicine 2020;37(4):269-276.
DOI: https://doi.org/10.12701/yujm.2020.00458
Published online: July 22, 2020
1Smart-Ageing Convergence Research Center, Yeungnam University College of Medicine, Daegu, Korea
2Department of Pharmacology, Yeungnam University College of Medicine, Daegu, Korea
3Department of Microbiology, Ewha Womans University College of Medicine, Seoul, Korea
- Corresponding authors: Chang-Hoon Woo Department of Pharmacology, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-640-6973 Fax: +82-53-656-7995 E-mail: changhoon_woo@yu.ac.kr
Copyright © 2020 Yeungnam University College of Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 9,413 Views
- 246 Download
- 4 Crossref
Abstract
- Fibrosis is characterized by excessive accumulation of extracellular matrix components. The fibrotic process ultimately leads to organ dysfunction and failure in chronic inflammatory and metabolic diseases such as pulmonary fibrosis, advanced kidney disease, and liver cirrhosis. Idiopathic pulmonary fibrosis (IPF) is a common form of progressive and chronic interstitial lung disease of unknown etiology. Pathophysiologically, the parenchyma of the lung alveoli, interstitium, and capillary endothelium becomes scarred and stiff, which makes breathing difficult because the lungs have to work harder to transfer oxygen and carbon dioxide between the alveolar space and bloodstream. The transforming growth factor beta (TGF-β) signaling pathway plays an important role in the pathogenesis of pulmonary fibrosis and scarring of the lung tissue. Recent clinical trials focused on the development of pharmacological agents that either directly or indirectly target kinases for the treatment of IPF. Therefore, to develop therapeutic targets for pulmonary fibrosis, it is essential to understand the key factors involved in the pathogenesis of pulmonary fibrosis and the underlying signaling pathway. The objective of this review is to discuss the role of kinase signaling cascades in the regulation of either TGF-β-dependent or other signaling pathways, including Rho-associated coiled-coil kinase, c-jun N-terminal kinase, extracellular signal-regulated kinase 5, and p90 ribosomal S6 kinase pathways, and potential therapeutic targets in IPF.
- Keywords: Fibrosis; Idiopathic pulmonary fibrosis; Kinase; Transforming growth factor beta
- Fibrosis is an excessive deposition of extracellular matrix (ECM) components, particularly fibrillar type I and III collagen [1,2]. Fibrosis is mainly driven by profibrogenic and proinflammatory cytokines, including the transforming growth factor beta (TGF-β) superfamily, tumor necrosis factor alpha (TNF-α), various interleukins, oxidative stress, and inflammation [3,4]. As a result, fibrosis can lead to failure of vital organs, including the lung, liver, heart, kidney, skin, and eye [5]. Pulmonary fibrosis is the final outcome of various parenchymal lung disorders, known as interstitial lung disease (ILD) [6]. One of the most common subtypes of ILD is idiopathic pulmonary fibrosis (IPF), which is a chronic, progressive, and generally fatal parenchymal lung disorder of unknown cause, with an approximate median survival of 2 to 5 years from diagnosis [7]. The clinical characteristics of IPF are heterogeneous and unpredictable, mainly including chronic cough, exertional dyspnea, declining lung function, and poor quality of life [8]. Epidemiological studies indicate that IPF is an age-related disease, and the majority of cases are diagnosed in patients over 60 years of age [9].
- The pathogenic mechanism in IPF is not clearly defined, but the disease is characterized by epithelial injury and activation, epithelial-mesenchymal transition (EMT), sustained fibroblast activation, and excessive ECM accumulation, which result in progressive and irrevocable distortion of the histological lung structure [10,11]. Previous studies have revealed the complex and vital role of TGF-β/Smad signaling in lung fibrosis [12-15]. Enhanced TGF-β1 signaling with excessive ECM accumulation has been reported in experimental models of pulmonary fibrosis as well as in human lung fibrotic tissue [16,17]. The inhibition of TGF-β by neutralizing anti-TGF-β antibody, decorin, RNA interference, or antisense oligonucleotides alleviates fibrosis [18-21]. Moreover, in a mouse model of bleomycin-induced pulmonary fibrosis, Smad3 deficiency attenuated pulmonary fibrosis [22]. TGF-β signaling can initiate both canonical Smad-dependent and Smad-independent signaling pathways [23]. In Smad-independent pathways, TGF-β activates the phosphoinositide 3-kinase (PI3K)/Akt pathway and mitogen-activated protein kinases (MAPKs) such as extracellular signal-regulated kinase (ERK) 1/2, p38, and c-jun N-terminal kinase (JNK) 1/2/3 [24].
- It has long been assumed that acute and chronic alveolitis lead to a fibrogenic response and play a critical role in the disease progression of IPF [25]. There are two different mechanisms involved in the pathogenesis of IPF. One of these is the ‘inflammatory pathway,’ which represents the major etiological pathway for IPF, associated with a marked collapse in the integrity of alveolar epithelial cells and subsequent fibrotic stage [25]. The other is the ‘epithelial/fibroblastic pathway,’ revealed by IPF [26]. These pathological changes, along with the disruption of the epithelial basement membrane enhance the migration of fibroblasts/myofibroblasts into the alveolar spaces and their subsequent deposition into the intra-alveolar ECM [26,27]. Many studies have shown that injured/activated alveolar epithelial cells in lungs from patients with IPF produce a variety of growth factors and pro-fibrotic cytokines [27,28].
Introduction
- Pirfenidone and nintedanib have been recently approved for the treatment of IPF [29-31]. Pirfenidone is a small molecule that inhibits inflammatory responses and the progression of fibrosis in experimental models and patients with IPF [32-34]. It downregulates the proliferation of fibroblasts and TGF-β1-induced collagen synthesis and reduces the production of the inflammatory cytokine TNF-α and interleukin-1β both in vitro and in vivo [35]. In a phase 3 study comparing pirfenidone with placebo in patients with IPF, pirfenidone treatment for 52 weeks significantly prolonged progression-free survival, compared with placebo [36]. In addition, with pirfenidone, there was a relative reduction of 47.9% in the proportion of patients who had a decline in predicted forced vital capacity or who died [36]. Pirfenidone is frequently associated with gastrointestinal adverse effects such as dyspepsia, nausea, and gastritis [37].
- Nintedanib is a small-molecule tyrosine kinase inhibitor targeting fibroblast growth factor receptor (FGFR) 1–3, vascular endothelial growth factor receptor (VEGFR) 1–3, and platelet-derived growth factor receptor (PDGFR) αβ, which are potentially involved in the progression of pulmonary fibrosis [38]. Nintedanib inhibits FGFR and PDGFR autophosphorylation and subsequent activation of downstream signaling via the Ras/Raf/MAPK, ERK1/2, and PI3K/Akt pathways [38]. Vascular endothelial growth factor (VEGF) stimulates angiogenesis through VEGFR and also binds to PDGFR in fibroblasts, subsequently stimulating cellular proliferation [38]. Nintedanib reduces migration, proliferation, and survival of fibroblasts, and ultimately attenuates angiogenesis in the lung [39]. In addition, administration of nintedanib attenuated the histopathological features of pulmonary fibrosis and expression of profibrogenic genes in experimental models of lung fibrosis [40]. In the two replicate phase 3 trials, nintedanib was shown to slow disease progression in patients with IPF by decreasing the annual rate of decline in forced vital capacity [41].
- Other recommendations for the pharmacological treatment of pulmonary fibrosis are warfarin, N-acetyl cysteine, imatinib, and endothelin receptor antagonists [9]. However, most clinical trials did not show significant differences between placebo and treatment effects in patients with IPF [9]. Therefore, there is still a need to develop new therapeutic targets and agents to inhibit the progression of pulmonary fibrosis and improve mortality rates.
Clinical treatment for pulmonary fibrosis
- 1. Receptor kinases
- In recent years, growth factors and receptor kinases have attracted attention as potential drug targets for pulmonary fibrosis. Several therapies targeting receptor kinases, including growth factor receptors, are currently in clinical trials for IPF (Table 1). Aberrantly activated lung epithelial cells are the primary source of TGF-β, fibroblast growth factor (FGF)-2, PDGF, connective tissue growth factor (CTGF), and endothelin-1, key factors in the development of IPF. Based on this evidence, clinical trials of nintedanib targeting multiple growth factor receptors could be successful. Additionally, several clinical trials of cytokine receptors, including TNF-α, interferon-γ, and interleukin-13, have been conducted with no significant impact in patients with IPF (NCT 02277145, NCT00532233, and NCT00075998).
- TGF-β mediates tissue fibrosis via recruitment and activation of monocytes and fibroblasts, and production of ECM through activation of serine/threonine kinase receptors [42,43]. In addition, TGF-β1 regulates the proliferation, differentiation, apoptosis, adhesion and migration, immunity, and even embryonic development, which ultimately contribute to fibrogenesis [44]. TGF-β has been shown to drive fibroblast-to-myofibroblast differentiation and directly promote pulmonary fibrosis in a mouse model of IPF [45]. Although TGF-β1 causes tissue fibrosis mainly by stimulating its downstream Smad signal transduction pathway, it is also known to activate Smad-independent signaling pathways, including MAPKs, focal adhesion kinase, and PI3K-Akt cascades in the pathogenesis of pulmonary fibrosis [46-48]. Both pharmacological and genetic inhibition of PI3K reduced pulmonary fibrosis in experimental rodent models, whereas overexpression of PI3K was observed in lung tissues from patients with IPF. A phase 1 clinical trial with a pharmacological inhibitor of PI3K is being conducted in healthy male and female subjects (NCT03502902).
- Drug development has been challenged by the problem of identifying selective pharmacological inhibitors of the TGF-β1 signaling pathway that function by inactivating either the ligand or receptor of TGF-β1. Since TGF-β family members are secreted in the form of inactive complexes with latency-associated peptide (LAP), which binds to integrin αVβ6, inhibition of the binding between αVβ6 and the LAP region of TGF-β1 has been considered as a potential strategy for drug development in IPF [49]. A couple of phase 2 clinical trials of an immunoglobulin G monoclonal antibody and a small-molecule inhibitor of integrin αVβ6 are being conducted in patients with IPF (NCT01371305 and NCT04396756). In addition, an inhalation formulation of a nucleic acid medicine that selectively suppresses the expression of TGF-β1 has been tested in a phase 1 clinical trial in patients with IPF (NCT03727802). In contrast to those of TGF-β ligand inhibition, there are no active clinical trials of direct inhibitors of TGF-β1 receptor in patients with IPF. There is, however, an ongoing phase 2 clinical trial of a galectin-3 inhibitor that indirectly suppresses TGF-β signaling via reduced cell surface expression of TGF-β receptors (NCT03832946) [50].
- CTGF, also known as cellular communication network factor 2, is a multifunctional growth factor that has been implicated in cell migration, proliferation, differentiation, and angiogenesis [51-54]. Since CTGF is an immediate early gene induced by TGF-β, PDGF, FGF-2, VEGF, and hypoxia, CTGF could regulate ECM deposition, tissue remodeling, and neovascularization, leading to the development of tissue fibrosis [55-58]. CTGF binds to integrin receptor α5β1 and induces the transactivation of FGFR2, PDGFR, and TGF-β receptor [59]. The fact that CTGF was elevated in lung fibrosis model and also in patients with IPF suggests its potential role in the treatment of IPF [60]. The neutralizing monoclonal antibody for CTGF has been shown to reduce lung fibrosis in experimental models [61,62]. A phase 3 clinical trial of a monoclonal antibody for CTGF is progressing in patients with IPF (NCT03955146).
- 2. Intracellular kinases
- Intracellular kinases are attractive targets for the treatment of IPF. There are a couple of clinical trials of inhibitors of the Rho-associated coiled-coil kinase (ROCK) and JNK (Table 1). The regulation of the actin cytoskeleton is a major feature of chronic fibrotic diseases implicating the wound healing process against tissue injury [63,64]. The ROCK family of serine/threonine kinases are key regulators of profibrotic processes and reasonable targets for a new therapeutic strategy for pulmonary fibrosis [65]. ROCK activation has been observed both in patients with IPF and in a mouse model of lung fibrosis, and pharmacological inhibition of ROCK protected mice from experimental lung fibrosis [66]. A phase 2 clinical trial of a pharmacological inhibitor of ROCK is ongoing in patients with IPF (NCT02688647) [67].
- It has been suggested that JNK activation in multiple cell types involved in lung fibrosis is positively correlated with the degree of fibrosis [68]. JNK1-deficient mice showed improved lung function in experimental models of lung fibrosis [69,70]. In a house dust mite model of lung fibrosis, a pharmacological JNK inhibitor decreased ECM accumulation and fibrosis [71,72]. A phase 2 clinical trial with a small-molecule inhibitor of JNK is being conducted in patients with IPF (NCT03142191).
Clinical trials with kinase inhibitors for idiopathic pulmonary fibrosis
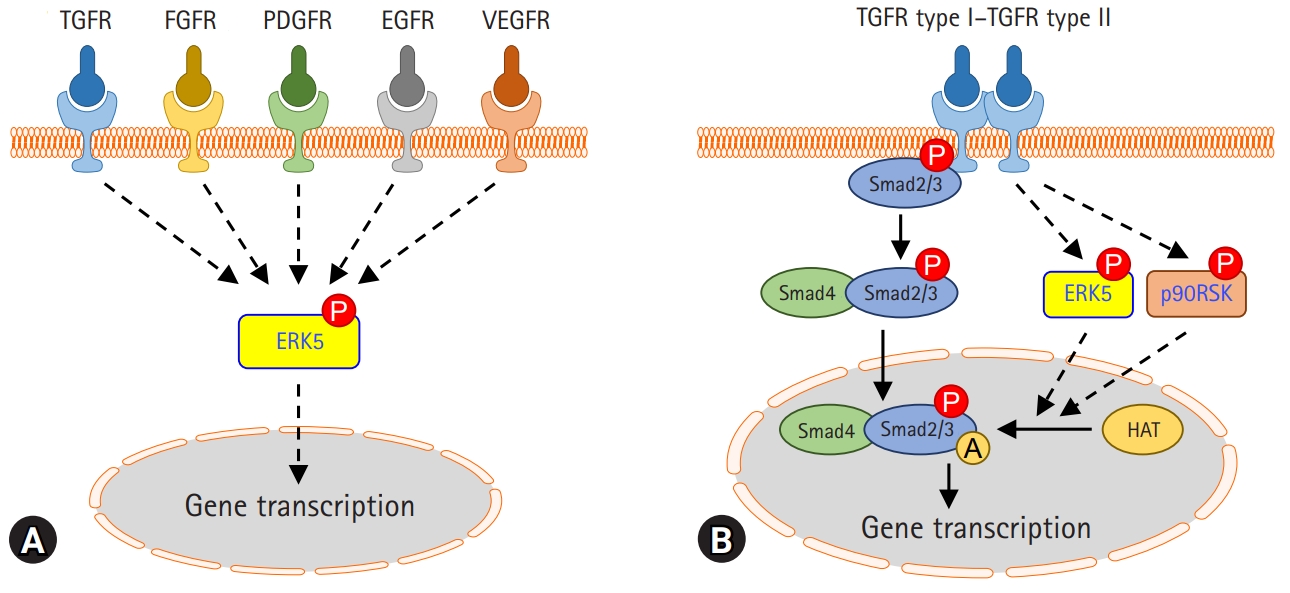
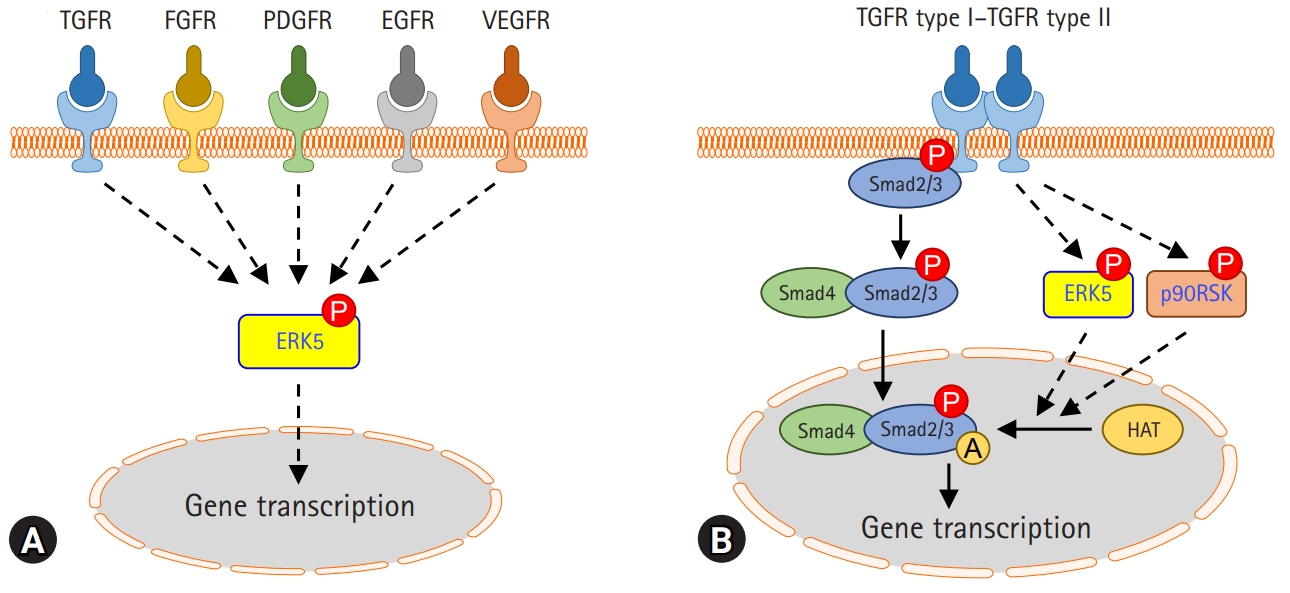
- A multitude of profibrotic mediators, including TGF-β, CTGF, PDGF, and FGF, and their signaling cascades, play an important role in the pathogenesis of fibrotic lung diseases. Collectively these signs of progress imply that kinase can be a good therapeutic target for pulmonary fibrosis. It has been shown that MAPK kinase (MEK) 1/2-ERK1/2-p90RSK inhibition reduces PDGF-AA-induced cellular migration [73]. FGF-2, a potent mitogen for fibroblasts, induces the synthesis of collagen in lung fibroblasts and myofibroblasts. Inhibition of ERK1/2 suppresses FGF-induced DNA synthesis, phosphorylation of ERK1/2, and p90RSK [74]. VEGF also causes rapid activation of Raf-1, MAPK, p90RSK in cardiac myocytes, and fibroblasts [75]. In addition, ERK5 modulates PDGF-induced proliferation and migration of hepatic stellate cells [76]. Many studies have revealed that ERK5 activation is induced by growth factors such as epidermal growth factor (EGF), FGF-2, and VEGF [77]. Thus, it is interesting that ERK5 is a common combined target for the treatment of pulmonary fibrosis through the regulation of growth factor signaling (Fig. 1A).
- ERK5 is an atypical member of the MAPK family and plays a critical role in hypertrophic cardiac remodeling via regulating fibrotic genes and ECM expression [78]. ERK5 is also involved in the enhancement of cell viability and ECM accumulation in chronic glomerulonephritis [79]. Since ERK5 could be activated by various growth factors affecting pulmonary fibrosis, it has been investigated whether ERK5 regulates TGF-β1-induced profibrotic responses and the pathogenesis of pulmonary fibrosis. Kim et al. [80] reported that pharmacological inhibition of MEK5/ERK5 with BIX02189 and depletion of ERK5 using small interfering RNA against ERK5 inhibited TGF-β1-induced ECM production and Smad3 transcriptional activity, but not Smad3 phosphorylation and nuclear translocation. Notably, it has been shown that ERK5 plays a vital role in TGF-β1-induced fibrogenic signaling via enhancing Smad3 acetylation [80]. Moreover, the pharmacological inhibition of ERK5 ameliorated lung fibrosis and improved survival rate in a mouse model of bleomycin-induced lung fibrosis [80]. This suggests that ERK5 may provide a potential therapeutic strategy to prevent the progression of pulmonary fibrosis (Fig. 1B).
- p90RSK is a family of serine/threonine kinases that is activated by the extracellular signal-regulated kinase signaling pathway. p90RSK is involved in numerous signal transduction and regulation of diverse cellular processes, including cell proliferation, growth, apoptosis, and transformation [81]. A recent study proposed that p90RSK is involved in the development and progression of liver fibrosis and hepatocellular injury in chronically damaged livers [82]. In addition, it has been reported that pharmacological inhibition of p90RSK using kaempferol inhibits TGF-β1-induced EMT and migration of A549 lung cancer cells [83]. A recent report showed that pharmacological inhibition of p90RSK by fluoromethyl ketone (FMK) or genetic inhibition of p90RSK significantly inhibited TGF-β1-induced Smad3 transcriptional activity, but not Smad3 phosphorylation and nuclear translocation [84]. In an experimental mouse model of bleomycin-induced lung fibrosis, p90RSK inhibitor FMK reduced pulmonary fibrosis, which suggests that it may be a novel therapeutic target for the treatment of lung fibrosis (Fig. 1B).
ERK5 and p90 ribosomal S6 kinase (p90RSK) in the fibrotic response
- Pulmonary fibrosis is a dreadful condition that demands urgent attention. Although TGF-β1 is known to play a critical role in the pathogenesis of pulmonary fibrosis, clinical trials of therapies targeting TGF-β are progressing through repeated failures. According to recent data, kinase inhibitors have been identified as reliable targets for developing therapeutic drugs to treat IPF through regulation of not only TGF-β signaling but also multiple kinase cascades. A couple of receptor kinases are progressing for clinical trials in patients with IPF. In addition to clinical trials, recent preclinical studies with an experimental mouse model of bleomycin-induced lung fibrosis in our group have suggested that pharmacological inhibition of ERK5 or p90RSK could be a potential target of pharmacological treatment of pulmonary fibrosis through inhibition of TGF-β-induced Smad3 transcriptional activation. Further intensive studies using selective kinase inhibitors are needed to develop therapeutic agents that might slow the progression of the disease and improve the prognosis of IPF.
Conclusion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This study was supported by the Basic Science Research Program (NRF-2018R1A2B6004664 to CHW, NRF-2018R1D1A1B07048399 to JHL) through the Korean National Research Foundation (NRF) funded by the Ministry of Science, ICT, and Future Planning, and by the Basic Science Research Program through the NRF funded by the Ministry of Education (NRF-2019R1I1A1A01060129 to SK).
-
Author contributions
Conceptualization, Investigation, Funding acquisition: all authors; Writing-original draft: SK; Writing-review & editing: JHL, CHW.
Notes
| Target molecule | Compound (type) | Mode of action | NCT ID (phase) |
|---|---|---|---|
| Multiple receptor kinases | Nintedaniba) (small-molecule) | Inhibit receptor kinases including PDGFR, FGFR, and VEGFR | Completed |
| TGF-β | BG00011 (IgG antibody) | Inhibit the activation of latent TGF-β via targeting integrin αVβ6 | NCT01371305 (2) |
| TGF-β | PLN-74809 (small-molecule) | Inhibit the activation of latent TGF-β via targeting αVβ1 and αVβ6 | NCT04396756 (2) |
| TGF-β | TRK-250 (nucleic acid) | Interfere the expression of TGF-β mRNA | NCT03727802 (1) |
| TGF-β receptor | TD139 (small-molecule) | Suppress the expression of TGFR via targeting galectin-3 | NCT03832946 (2) |
| CTGF | Pamrevlumab (IgG antibody) | Interfere CTGF bioavailability and subsequent receptor signaling | NCT03955146 (3) |
| ROCK | KD025 (small-molecule) | Inhibit ROCK | NCT02688647 (2) |
| JNK | CC-90001 (small-molecule) | Inhibit JNK | NCT03142191 (2) |
NCT ID, national clinical trial identifier number from ClinicalTrials.gov; PDGFR, platelet-derived growth factor receptor; FGFR, fibroblast growth factor receptor; VEGFR, vascular endothelial growth factor receptor; TGF-β, transforming growth factor beta; mRNA, messenger RNA; TGFR, transforming growth factor receptor; CTGF, connective tissue growth factor; IgG, immunoglobulin G; ROCK, Rho-associated coiled-coil protein kinase; JNK, c-jun N-terminal kinase.
a) U.S. Food and Drug Administration approved.
- 1. Bonnans C, Chou J, Werb Z. Remodelling the extracellular matrix in development and disease. Nat Rev Mol Cell Biol 2014;15:786–801.ArticlePubMedPMCPDF
- 2. Iredale JP, Thompson A, Henderson NC. Extracellular matrix degradation in liver fibrosis: biochemistry and regulation. Biochim Biophys Acta 2013;1832:876–83.ArticlePubMed
- 3. Borthwick LA, Wynn TA, Fisher AJ. Cytokine mediated tissue fibrosis. Biochim Biophys Acta 2013;1832:1049–60.ArticlePubMed
- 4. Liu RM, Gaston Pravia KA. Oxidative stress and glutathione in TGF-beta-mediated fibrogenesis. Free Radic Biol Med 2010;48:1–15.ArticlePubMed
- 5. Rockey DC, Bell PD, Hill JA. Fibrosis: a common pathway to organ injury and failure. N Engl J Med 2015;372:1138–49.ArticlePubMed
- 6. King TE Jr. Clinical advances in the diagnosis and therapy of the interstitial lung diseases. Am J Respir Crit Care Med 2005;172:268–79.ArticlePubMed
- 7. Strongman H, Kausar I, Maher TM. Incidence, prevalence, and survival of patients with idiopathic pulmonary fibrosis in the UK. Adv Ther 2018;35:724–36.ArticlePubMedPMCPDF
- 8. Hopkins RB, Burke N, Fell C, Dion G, Kolb M. Epidemiology and survival of idiopathic pulmonary fibrosis from national data in Canada. Eur Respir J 2016;48:187–95.ArticlePubMed
- 9. Raghu G. Idiopathic pulmonary fibrosis: lessons from clinical trials over the past 25 years. Eur Respir J 2017;50:1701209.ArticlePubMed
- 10. Noble PW, Homer RJ. Idiopathic pulmonary fibrosis: new insights into pathogenesis. Clin Chest Med 2004;25:749–58.ArticlePubMed
- 11. Thannickal VJ, Toews GB, White ES, Lynch JP 3rd, Martinez FJ. Mechanisms of pulmonary fibrosis. Annu Rev Med 2004;55:395–417.ArticlePubMed
- 12. Saito A, Horie M, Nagase T. TGF-β signaling in lung health and disease. Int J Mol Sci 2018;19:2460.ArticlePubMedPMC
- 13. Flanders KC. Smad3 as a mediator of the fibrotic response. Int J Exp Pathol 2004;85:47–64.ArticlePubMedPMC
- 14. Nakerakanti S, Trojanowska M. The role of TGF-β receptors in fibrosis. Open Rheumatol J 2012;6:156–62.ArticlePubMedPMC
- 15. Gordon KJ, Blobe GC. Role of transforming growth factor-beta superfamily signaling pathways in human disease. Biochim Biophys Acta 2008;1782:197–228.ArticlePubMed
- 16. Hoyt DG, Lazo JS. Alterations in pulmonary mRNA encoding procollagens, fibronectin and transforming growth factor-beta precede bleomycin-induced pulmonary fibrosis in mice. J Pharmacol Exp Ther 1988;246:765–71.PubMed
- 17. Broekelmann TJ, Limper AH, Colby TV, McDonald JA. Transforming growth factor beta 1 is present at sites of extracellular matrix gene expression in human pulmonary fibrosis. Proc Natl Acad Sci U S A 1991;88:6642–6.ArticlePubMedPMC
- 18. Wu CF, Chiang WC, Lai CF, Chang FC, Chen YT, Chou YH, et al. Transforming growth factor β-1 stimulates profibrotic epithelial signaling to activate pericyte-myofibroblast transition in obstructive kidney fibrosis. Am J Pathol 2013;182:118–31.ArticlePubMedPMC
- 19. Border WA, Noble NA, Yamamoto T, Harper JR, Yamaguchi Yu, Pierschbacher MD, et al. Natural inhibitor of transforming growth factor-beta protects against scarring in experimental kidney disease. Nature 1992;360:361–4.ArticlePubMedPDF
- 20. Isaka Y, Tsujie M, Ando Y, Nakamura H, Kaneda Y, Imai E, et al. Transforming growth factor-beta 1 antisense oligodeoxynucleotides block interstitial fibrosis in unilateral ureteral obstruction. Kidney Int 2000;58:1885–92.ArticlePubMed
- 21. Takabatake Y, Isaka Y, Mizui M, Kawachi H, Shimizu F, Ito T, et al. Exploring RNA interference as a therapeutic strategy for renal disease. Gene Ther 2005;12:965–73.ArticlePubMedPDF
- 22. Zhao J, Shi W, Wang YL, Chen H, Bringas P Jr, Datto MB, et al. Smad3 deficiency attenuates bleomycin-induced pulmonary fibrosis in mice. Am J Physiol Lung Cell Mol Physiol 2002;282:L585–93.ArticlePubMed
- 23. Zi Z, Chapnick DA, Liu X. Dynamics of TGF-β/Smad signaling. FEBS Lett 2012;586:1921–8.ArticlePubMedPMC
- 24. Zhang YE. Non-Smad pathways in TGF-beta signaling. Cell Res 2009;19:128–39.ArticlePubMedPMCPDF
- 25. Bringardner BD, Baran CP, Eubank TD, Marsh CB. The role of inflammation in the pathogenesis of idiopathic pulmonary fibrosis. Antioxid Redox Signal 2008;10:287–301.ArticlePubMedPMC
- 26. Selman M, Pardo A. Idiopathic pulmonary fibrosis: an epithelial/fibroblastic cross-talk disorder. Respir Res 2002;3:3.ArticlePubMed
- 27. Sakai N, Tager AM. Fibrosis of two: epithelial cell-fibroblast interactions in pulmonary fibrosis. Biochim Biophys Acta 2013;1832:911–21.ArticlePubMedPMC
- 28. Camelo A, Dunmore R, Sleeman MA, Clarke DL. The epithelium in idiopathic pulmonary fibrosis: breaking the barrier. Front Pharmacol 2014;4:173.ArticlePubMedPMC
- 29. Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med 2014;370:2071–82.ArticlePubMed
- 30. Ogura T, Taniguchi H, Azuma A, Inoue Y, Kondoh Y, Hasegawa Y, et al. Safety and pharmacokinetics of nintedanib and pirfenidone in idiopathic pulmonary fibrosis. Eur Respir J 2015;45:1382–92.ArticlePubMed
- 31. Taniguchi H, Ebina M, Kondoh Y, Ogura T, Azuma A, Suga M, et al. Pirfenidone in idiopathic pulmonary fibrosis. Eur Respir J 2010;35:821–9.ArticlePubMed
- 32. Gurujeyalakshmi G, Hollinger MA, Giri SN. Pirfenidone inhibits PDGF isoforms in bleomycin hamster model of lung fibrosis at the translational level. Am J Physiol 1999;276:L311–8.ArticlePubMed
- 33. Iyer SN, Gurujeyalakshmi G, Giri SN. Effects of pirfenidone on transforming growth factor-beta gene expression at the transcriptional level in bleomycin hamster model of lung fibrosis. J Pharmacol Exp Ther 1999;291:367–73.PubMed
- 34. Noble PW, Albera C, Bradford WZ, Costabel U, Glassberg MK, Kardatzke D, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet 2011;377:1760–9.ArticlePubMed
- 35. Lopez-de la Mora DA, Sanchez-Roque C, Montoya-Buelna M, Sanchez-Enriquez S, Lucano-Landeros S, Macias-Barragan J, et al. Role and new insights of pirfenidone in fibrotic diseases. Int J Med Sci 2015;12:840–7.ArticlePubMedPMC
- 36. King TE Jr, Bradford WZ, Castro-Bernardini S, Fagan EA, Glaspole I, Glassberg MK, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med 2014;370:2083–92.ArticlePubMed
- 37. Jiang C, Huang H, Liu J, Wang Y, Lu Z, Xu Z. Adverse events of pirfenidone for the treatment of pulmonary fibrosis: a meta-analysis of randomized controlled trials. PLoS One 2012;7:e47024.ArticlePubMedPMC
- 38. Wollin L, Wex E, Pautsch A, Schnapp G, Hostettler KE, Stowasser S, et al. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur Respir J 2015;45:1434–45.ArticlePubMedPMC
- 39. Hostettler KE, Zhong J, Papakonstantinou E, Karakiulakis G, Tamm M, Seidel P, et al. Anti-fibrotic effects of nintedanib in lung fibroblasts derived from patients with idiopathic pulmonary fibrosis. Respir Res 2014;15:157.ArticlePubMedPMCPDF
- 40. Wollin L, Maillet I, Quesniaux V, Holweg A, Ryffel B. Antifibrotic and anti-inflammatory activity of the tyrosine kinase inhibitor nintedanib in experimental models of lung fibrosis. J Pharmacol Exp Ther 2014;349:209–20.ArticlePubMed
- 41. Richeldi L, Cottin V, Flaherty KR, Kolb M, Inoue Y, Raghu G, et al. Design of the INPULSIS™ trials: two phase 3 trials of nintedanib in patients with idiopathic pulmonary fibrosis. Respir Med 2014;108:1023–30.ArticlePubMed
- 42. Meng XM, Nikolic-Paterson DJ, Lan HY. TGF-β: the master regulator of fibrosis. Nat Rev Nephrol 2016;12:325–38.ArticlePubMedPDF
- 43. Choi ME. Mechanism of transforming growth factor-β1 signaling: role of the mitogen-activated protein kinase. Kidney Int 2000;58(Suppl 77):S53–8.Article
- 44. Leask A, Abraham DJ. All in the CCN family: essential matricellular signaling modulators emerge from the bunker. J Cell Sci 2006;119(Pt 23):4803–10.ArticlePubMed
- 45. Yue X, Shan B, Lasky JA. TGF-β: titan of lung fibrogenesis. Curr Enzym Inhib 2010;6:10.2174/10067.ArticlePMC
- 46. Varga J, Abraham D. Systemic sclerosis: a prototypic multisystem fibrotic disorder. J Clin Invest 2007;117:557–67.ArticlePubMedPMC
- 47. Derynck R, Zhang YE. Smad-dependent and Smad-independent pathways in TGF-beta family signalling. Nature 2003;425:577–84.ArticlePubMedPDF
- 48. Das F, Ghosh-Choudhury N, Venkatesan B, Li X, Mahimainathan L, Choudhury GG. Akt kinase targets association of CBP with SMAD 3 to regulate TGFbeta-induced expression of plasminogen activator inhibitor-1. J Cell Physiol 2008;214:513–27.ArticlePubMed
- 49. Munger JS, Huang X, Kawakatsu H, Griffiths MJD, Dalton SL, Wu J, et al. The integrin αvβ6 binds and activates latent TGFβ1: a mechanism for regulating pulmonary inflammation and fibrosis. Cell 1999;96:319–28.ArticlePubMed
- 50. Mackinnon AC, Gibbons MA, Farnworth SL, Leffler H, Nilsson UJ, Delaine T, et al. Regulation of transforming growth factor-β1-driven lung fibrosis by galectin-3. Am J Respir Crit Care Med 2012;185:537–46.ArticlePubMedPMC
- 51. Brigstock DR. The connective tissue growth factor/cysteine-rich 61/nephroblastoma overexpressed (CCN) family. Endocr Rev 1999;20:189–206.ArticlePubMed
- 52. Kondo S, Kubota S, Shimo T, Nishida T, Yosimichi G, Eguchi T, et al. Connective tissue growth factor increased by hypoxia may initiate angiogenesis in collaboration with matrix metalloproteinases. Carcinogenesis 2002;23:769–76.ArticlePubMedPDF
- 53. Shimo T, Nakanishi T, Nishida T, Asano M, Sasaki A, Kanyama M, et al. Involvement of CTGF, a hypertrophic chondrocyte-specific gene product, in tumor angiogenesis. Oncology 2001;61:315–22.ArticlePubMed
- 54. Takigawa M. CTGF/Hcs24 as a multifunctional growth factor for fibroblasts, chondrocytes and vascular endothelial cells. Drug News Perspect 2003;16:11–21.ArticlePubMed
- 55. Igarashi A, Okochi H, Bradham DM, Grotendorst GR. Regulation of connective tissue growth factor gene expression in human skin fibroblasts and during wound repair. Mol Biol Cell 1993;4:637–45.ArticlePubMedPMC
- 56. Grotendorst GR, Okochi H, Hayashi N. A novel transforming growth factor beta response element controls the expression of the connective tissue growth factor gene. Cell Growth Differ 1996;7:469–80.PubMed
- 57. Shimo T, Kubota S, Kondo S, Nakanishi T, Sasaki A, Mese H, et al. Connective tissue growth factor as a major angiogenic agent that is induced by hypoxia in a human breast cancer cell line. Cancer Lett 2001;174:57–64.ArticlePubMed
- 58. Suzuma K, Naruse K, Suzuma I, Takahara N, Ueki K, Aiello LP, et al. Vascular endothelial growth factor induces expression of connective tissue growth factor via KDR, Flt1, and phosphatidylinositol 3-kinase-akt-dependent pathways in retinal vascular cells. J Biol Chem 2000;275:40725–31.ArticlePubMed
- 59. Lau LF. Cell surface receptors for CCN proteins. J Cell Commun Signal 2016;10:121–7.ArticlePubMedPMCPDF
- 60. Wang Q, Usinger W, Nichols B, Gray J, Xu L, Seeley TW, et al. Cooperative interaction of CTGF and TGF-β in animal models of fibrotic disease. Fibrogenesis Tissue Repair 2011;4:4.ArticlePubMedPMC
- 61. Kono M, Nakamura Y, Suda T, Kato M, Kaida Y, Hashimoto D, et al. Plasma CCN2 (connective tissue growth factor; CTGF) is a potential biomarker in idiopathic pulmonary fibrosis (IPF). Clin Chim Acta 2011;412:2211–5.ArticlePubMed
- 62. Pan LH, Yamauchi K, Uzuki M, Nakanishi T, Takigawa M, Inoue H, et al. Type II alveolar epithelial cells and interstitial fibroblasts express connective tissue growth factor in IPF. Eur Respir J 2001;17:1220–7.ArticlePubMed
- 63. Gabbiani G. Modulation of fibroblastic cytoskeletal features during wound healing and fibrosis. Pathol Res Pract 1994;190:851–3.ArticlePubMed
- 64. Sandbo N, Dulin N. Actin cytoskeleton in myofibroblast differentiation: ultrastructure defining form and driving function. Transl Res 2011;158:181–96.ArticlePubMedPMC
- 65. Knipe RS, Tager AM, Liao JK. The Rho kinases: critical mediators of multiple profibrotic processes and rational targets for new therapies for pulmonary fibrosis. Pharmacol Rev 2015;67:103–17.ArticlePubMedPMC
- 66. Zhou Y, Huang X, Hecker L, Kurundkar D, Kurundkar A, Liu H, et al. Inhibition of mechanosensitive signaling in myofibroblasts ameliorates experimental pulmonary fibrosis. J Clin Invest 2013;123:1096–108.ArticlePubMedPMC
- 67. Griffith DE, Eagle G, Thomson R, Aksamit TR, Hasegawa N, Morimoto K, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT): a prospective, open-label, randomized study. Am J Respir Crit Care Med 2018;198:1559–69.ArticlePubMed
- 68. Yoshida K, Kuwano K, Hagimoto N, Watanabe K, Matsuba T, Fujita M, et al. MAP kinase activation and apoptosis in lung tissues from patients with idiopathic pulmonary fibrosis. J Pathol 2002;198:388–96.ArticlePubMed
- 69. Alcorn JF, van der Velden J, Brown AL, McElhinney B, Irvin CG, Janssen-Heininger YM. c-Jun N-terminal kinase 1 is required for the development of pulmonary fibrosis. Am J Respir Cell Mol Biol 2009;40:422–32.ArticlePubMed
- 70. Van der Velden JL, Alcorn JF, Chapman DG, Lundblad LK, Irvin CG, Davis RJ, et al. Airway epithelial specific deletion of Jun-N-terminal kinase 1 attenuates pulmonary fibrosis in two independent mouse models. PLoS One 2020;15:e0226904.ArticlePubMedPMC
- 71. Bennett B, Blease K, Ye Y, Azaryan A, Ramirez-Valle F, Ceres R, et al. CC-90001, a second generation Jun N-terminal kinase (JNK) inhibitor for the treatment of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 2017;195:A5409.
- 72. Van der Velden JL, Ye Y, Nolin JD, Hoffman SM, Chapman DG, Lahue KG, et al. JNK inhibition reduces lung remodeling and pulmonary fibrotic systemic markers. Clin Transl Med 2016;5:36.ArticlePubMedPMC
- 73. Clement DL, Mally S, Stock C, Lethan M, Satir P, Schwab A, et al. PDGFRα signaling in the primary cilium regulates NHE1-dependent fibroblast migration via coordinated differential activity of MEK1/2-ERK1/2-p90RSK and AKT signaling pathways. J Cell Sci 2013;126(Pt 4):953–65.ArticlePubMedPMC
- 74. Delehedde M, Seve M, Sergeant N, Wartelle I, Lyon M, Rudland PS, et al. Fibroblast growth factor-2 stimulation of p42/44MAPK phosphorylation and IkappaB degradation is regulated by heparan sulfate/heparin in rat mammary fibroblasts. J Biol Chem 2000;275:33905–10.ArticlePubMed
- 75. Seko Y, Takahashi N, Tobe K, Ueki K, Kadowaki T, Yazaki Y. Vascular endothelial growth factor (VEGF) activates Raf-1, mitogen-activated protein (MAP) kinases, and S6 kinase (p90rsk) in cultured rat cardiac myocytes. J Cell Physiol 1998;175:239–46.ArticlePubMed
- 76. Rovida E, Navari N, Caligiuri A, Dello Sbarba P, Marra F. ERK5 differentially regulates PDGF-induced proliferation and migration of hepatic stellate cells. J Hepatol 2008;48:107–15.ArticlePubMed
- 77. Roberts OL, Holmes K, Muller J, Cross DA, Cross MJ. ERK5 and the regulation of endothelial cell function. Biochem Soc Trans 2009;37(Pt 6):1254–9.ArticlePubMedPDF
- 78. Kimura TE, Jin J, Zi M, Prehar S, Liu W, Oceandy D, et al. Targeted deletion of the extracellular signal-regulated protein kinase 5 attenuates hypertrophic response and promotes pressure overload-induced apoptosis in the heart. Circ Res 2010;106:961–70.ArticlePubMedPMC
- 79. Urushihara M, Takamatsu M, Shimizu M, Kondo S, Kinoshita Y, Suga K, et al. ERK5 activation enhances mesangial cell viability and collagen matrix accumulation in rat progressive glomerulonephritis. Am J Physiol Renal Physiol 2010;298:F167–76.ArticlePubMed
- 80. Kim S, Lim JH, Woo CH. ERK5 inhibition ameliorates pulmonary fibrosis via regulating Smad3 acetylation. Am J Pathol 2013;183:1758–68.ArticlePubMed
- 81. Frodin M, Gammeltoft S. Role and regulation of 90 kDa ribosomal S6 kinase (RSK) in signal transduction. Mol Cell Endocrinol 1999;151:65–77.ArticlePubMed
- 82. Morales-Ibanez O, Affo S, Rodrigo-Torres D, Blaya D, Millan C, Coll M, et al. Kinase analysis in alcoholic hepatitis identifies p90RSK as a potential mediator of liver fibrogenesis. Gut 2016;65:840–51.ArticlePubMed
- 83. Jo E, Park SJ, Choi YS, Jeon WK, Kim BC. Kaempferol suppresses transforming growth factor-β1-induced epithelial-to-mesenchymal transition and migration of A549 lung cancer cells by inhibiting akt1-mediated phosphorylation of Smad3 at threonine-179. Neoplasia 2015;17:525–37.ArticlePubMedPMC
- 84. Kim S, Han JH, Kim S, Lee H, Kim JR, Lim JH, et al. p90RSK inhibition ameliorates TGF-β1 signaling and pulmonary fibrosis by inhibiting Smad3 transcriptional activity. Cell Physiol Biochem 2020;54:195–210.ArticlePubMed
References
Figure & Data
References
Citations
- Targeting Growth Factor and Cytokine Pathways to Treat Idiopathic Pulmonary Fibrosis
Hongbo Ma, Shengming Liu, Shanrui Li, Yong Xia
Frontiers in Pharmacology.2022;[Epub] CrossRef - Vitamin D3 alleviates pulmonary fibrosis by regulating the MAPK pathway via targeting PSAT1 expression in vivo and in vitro
Wenxiang Zhu, Qi Ding, Lu Wang, Gonghao Xu, Yirui Diao, Sihao Qu, Sheng Chen, Yuanyuan Shi
International Immunopharmacology.2021; 101: 108212. CrossRef - Advances in the science and treatment of respiratory diseases
Jin Hong Chung
Yeungnam University Journal of Medicine.2020; 37(4): 251. CrossRef - Effects of Pirfenidone and Nintedanib on Markers of Systemic Oxidative Stress and Inflammation in Patients with Idiopathic Pulmonary Fibrosis: A Preliminary Report
Alessandro G. Fois, Elisabetta Sotgiu, Valentina Scano, Silvia Negri, Sabrina Mellino, Elisabetta Zinellu, Pietro Pirina, Gianfranco Pintus, Ciriaco Carru, Arduino A. Mangoni, Angelo Zinellu
Antioxidants.2020; 9(11): 1064. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite